
Neuromuscular Examination Elements
PTA 204L Neurological Dysfunctions Lab
The following information is used for instructional purposes for students enrolled in the Physical Therapist Assistant Program at Lane Community College. It is not intended for commercial use or distribution or commercial purposes. It is not intended to serve as medical advice or treatment.
Contact howardc@lanecc.edu for permissions.
Movies drawn from the Neurologic Exam and PediNeurologic Exam web sites are used by permission of Paul D. Larsen, M.D., University of Nebraska Medical Center and Suzanne S. Stensaas, Ph.D., University of Utah School of Medicine. Additional materials for Neurologic Exam are drawn from resources provided by Alejandro Stern, Stern Foundation, Buenos Aires, Argentina; Kathleen Digre, M.D., University of Utah; and Daniel Jacobson, M.D., Marshfield Clinic, Wisconsin. Subsequent re-use of any materials outside of this program, presentation, or website requires permission from the original producers.
Each physical therapist develops and individualized flow of examination. The Guide to Physical Therapist Practice provides a framework for the key elements of a comprehensive neuromuscular examination. Family members, care givers, staff, and patients will have questions about terminology, function, and functional deficits.
Major components of a neuromuscular system examination include:
These specific examination findings lead the PT to form primary and secondary PT diagnoses, and impairments and limitations that will be addressed with selected interventions. Impairments of the neuromuscular system can lead to changes in musculoskeletal, cardiovascular, pulmonary and integument systems. For example, loss of sensation and active ROM from a CVA can lead to pressure ulcers from malpositioning, contractures and joint dysfunction from abnormal use/disuse of an extremity, decreased endurance from changes in physical activity, and loss of respiratory capacity from changes in trunk strength.
A PT applies knowledge of neuropathology, motor learning, and body systems to examination findings and develops a prognosis, plan of care, and goals that reflect the patients needs and situation.
The linked handout to the right includes some key terms used in documentation for patients with neurological dysfunction. Download the handout on the right as a supplemental resource to aid your understanding of neurological terms.
A video example of history taking is available in your textbook resources at: http://www.healio.com/books/sites/neuroptavideos/chapter-5.
"Learning to listen" shows how history-taking with the patient can lend insight in to orientation, memory, and motivation. Additionally, history is derived from the medical record, trusted family, friends, teachers and caregivers, lab and imaging outcomes, and prior encounters with the patients.
During the patient interview, the therapist can also note speech production and speech deficits associated with neurological dysfunction. It is important to document and discriminate speech disorders and impacts on command-following, comprehension, and problem-solving prior to initiating treatment.
Until recently, pain was referred to as the fifth vital sign. Patients should be interviewed about their pain experience during the examination and treatment processes.
Pain assessment tool selection depends on cognitive status and language function. Primitive withdrawal reflexes, grimacing, or vocalizing may be the only modalities available for your patient to express and respond to painful stimuli. Observations are pivotal in assessing pain and potential risk for injury during physical therapy interventions. Common assessment tools in this patient population include the Visual Analog Scale (VAS), Faces Pain Scale (FPS), and body diagrams. Other standardized tools are available to reliably gather information from non-verbal patients about their pain experience, including infants
http://boneandspine.com/wp-content/uploads/2013/08/faces-pain-scale-revised.png
In PTA 103L, we practiced assessing A&O status during case simulation. We also practiced using some standardized screening/assessment tools for documenting memory function and information processing. If you'd like to refresh your understanding of language and tools used to assess and document mental function, the PTA 103L A&O activity is available for download on the right.
The videos below demonstrate techniques to assess cognitive status. Compare the outcomes of the normal exam with the abnormal exam. What key differences do you notice?
By reviewing the linked videos, you will prepare for patient communication in skill checks, lab exams and in the clinic.
Normal Orientation and Memory
Abnormal Orientation and Memory
Speech and language deficits may be confused with impaired memory. Individuals who have difficult processing or producing language may have difficulty responding reliably to verbal and/or written questions designed to assess orientation. Speech intelligibility (dysarthria, apraxia) may be decreased when there is weakness of facial muscles, decreased coordination during word/sound formation, or poor breath support during speech. Aphasia describes central losses of language.
Normal Receptive Language
Receptive Aphasia - Abnormal Receptive Language
This speech pattern may also be referred to as "word salad". Receptive patterns can result in nonsense words and disconnected and repetitive phrases. Patients are unable to detect errors in their own speech, therefore, communication and comprehension is significantly impaired. In the "More Resources" link on this page, you can read a sample of a "word salad" exchange from an episode of "Boston Legal"
Normal Expressive Language
Expressive Aphasia - Abnormal Expressive Language
Expressive deficits are characterized by errors in speech production. In general, patients are able to understand speech and commands/requests, yet their responses are incorrect or incomplete. Patients are often aware of their errors in speech production, which can result in frustration and depression.
PTAs can coordinate with health care team members, including Speech and Language Pathologists, to facilitate positive and productive reciprocal communication during therapy sessions and family training.
Sensory testing provides valuable information about how information from the outside world and information from the skin and joints is integrated by the nervous system. Sensory testing is used frequently to gauge recovery of cortical systems as well as peripheral nerve function.
Recall from PTA 103L your practice in assessing light touch sensation in the upper and lower extremities. Using a light cotton swab or tissue, you were able to correctly assess light touch by referencing dermatome maps and relating it sensory processing at a specific spinal level. You may wish to review the spinal levels and their respective dermatomes to refresh your memory of this relationship.
Link to LCC PTA Program Sensory Dance Video
Testing sensation in this patient population becomes more specialized beyond those tests learned in PTA 103L. Course readings (Umphred, Chapter 5) describe and summarize the multiple tests which are performed to differentiate sensory function. In this course, we will demonstrate and practice tests for joint position sense (proprioception) and joint motion (kinesthesia)
Demonstration of sensory testing procedures for your skill check are included in: Somatosensory Examination Tutorial.
Basic assessment of motor function include ROM, strength, and tone. Integration sensorimotor function allows the therapist to assess more complex and integrated functional motor responses, such as coordination, timing , accuracy, and balance. Any evidence of abnormal synergies (flexion/extension) during movement is observed and documented
This video provides a simulated example of hemiparetic gait, integrating stereotypical flexion synergies in the affected UE and extension synergies in the affected LE.
PTs will assess gross coordination of head and eye movements, limb movements, and trunk and limb coordination as part of the initial examination. Basic postural control hinges on the interactions of the CNS, vestibular, visual, and musculoskeletal systems. Recall that the primary function of the cerebellum is for muscle timing and force, error correction, and coordination of movements. Patients with disorders affecting the cerebellum will present with coordination deficits.
Common coordination tests are available in your Umphred text. See page 134 for a summary of tests which may be selected during a PT examination. Videos are linked below to provide you with examples of abnormal coordination.
Dysdiadochokinesia
Abnormal Alternate Nose - to - Finger test
Abnormal Heel - to - Shin test
Coordination tests for nose-finger-nose, rapid alternating movement and heel-to-shin are demonstrated in the 'Coordination and Balance' section of this lecture and described in your Umphred text (p. 134).
Practice performing these tests after viewing the demonstrations provided in "Coordination and Balance". Course readings will support your practice. Include in your practice expectations of processing delays, language impairments (aphasia), and visual neglects so you are practicing in the context of the clinical setting where these tests are most often performed.
Balance testing includes static ("quiet") and dynamic sitting and standing balance. Functional activities are often included in balance assessment to help describe the impact of poor trunk control and delayed balance responses with everyday activities. Alignment, responses to perturbations, visual disturbance, and weight-bearing surface allow for differential PT diagnosis and prioritized treatment planning.
Cranial nerves are the pathways to perception of
•Olfaction
•Taste
•Visual system
•Hearing and balance
Cranial nerves reside in throughout the brain: cerebrum, and brain stem (midbrain, pons, and medulla oblongota). PTs will screen and assess gross cranial nerve function through observation of involuntary movement and simple motor commands.
Brainstem: connects spinal cord to brain; integration of reflexes necessary for survival
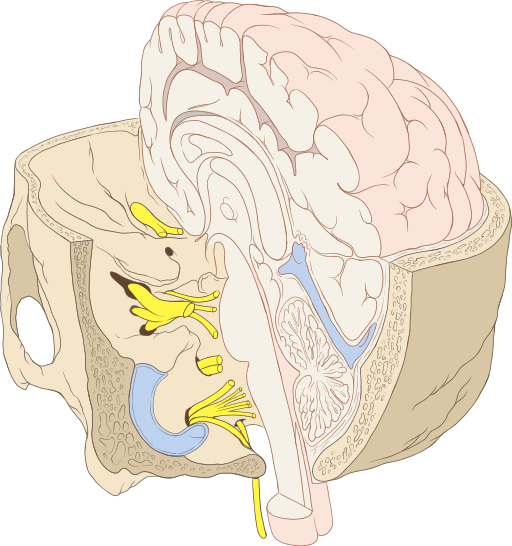
By Patrick J. Lynch, medical illustrator (Patrick J. Lynch, medical illustrator) [CC-BY-2.5 (http://creativecommons.org/licenses/by/2.5)], via Wikimedia Commons
Cranial nerves (CN): part of peripheral nervous system which arises directly from brain. Two pairs of CN arise from cerebrum; ten pairs arise from brainstem. Indicated by
Roman numerals I-XII from anterior to posterior. CNs may have one or more of three functions
|
Brain Subdivision |
Associated Cranial Nerve |
Major Function |
|
cerebrum |
I: Olfactory |
Smell and taste |
|
thalamus |
II: Optic |
Vision |
|
midbrain |
III: Oculomotor IV: Trochlear |
Eye movements (adduction, elevation, depression) and motor for eyelid |
|
pons |
V: Trigeminal VI: Abducens VII: Facial VIII: Vestibulocochlear(part) |
Face sensation and motor Lateral eye movement Face sensory and motor, taste
Hearing and balance |
|
medulla oblongata |
VIII: Vestibulocochlear (part) IX: Glossopharyngeal X: Vagus
XI: Spinal Accessory XII: Hypoglossal |
Hearing and balance
Taste posterior third of tongue and sensory/motor in throat Autonomic functions for viscera, (BP, HR, RR), speech, breathing Motor to SCM and trapezius Motor function for tongue |
The Wayne State Tutorial is highly detailed and includes a section on "interpretation" which is outside of the PTA scope of practice. We have narrowed the focused of the tutorial by linking the procedures for testing in the table below.
Any patient who reports and/or demonstrates new signs and symptoms of cranial nerve dysfunction may be experiencing a medical emergency.
A PTA should be able to select and perform tests for cranial nerve function. Specific cranial nerve testing procedures are linked below:
|
Cranial Nerve |
Procedures |
Video Demo of Normal Function |
|
I - Olfactory |
Testing Smell |
Smell test video |
|
II - Optic |
Testing Visual Fields |
Visual field test demo |
|
III, IV, VI - Eye control |
Tracking Saccades Convergence Divergence |
Eye motor control test demo |
|
V - Trigeminal |
Testing face sensation |
Face sensation and motor test demo |
|
VII- Facial |
Testing face muscles |
Facial motor testing and taste demo |
|
VIII - Vestibulocochlear |
Testing hearing function Testing vestibular function |
Hearing function test demo |
|
IX, X - Gag Reflexes |
Testing gag reflex Testing vocal motor function |
Gag reflex testing demo |
|
XI - Spinal Accessory |
Testing Trapezius and SCM function |
Manual muscle testing demo |
|
XII - Hypoglossal |
Testing tongue movements |
Tongue strength and motion testing demo |
For your reference, you can link to the full Wayne State Cranial Nerve Tutorial
Abnormal Cranial Nerve II
Recall that visual fields are dependent on individual eye function as well as convergence of both eyes on an object/image. Damage to central visual processing systems can result in visual disturbances or field cuts.
|
Full Visual Field - Binocular Vision |
Left Visual Field Cut |
|
|
|
http://en.wikipedia.org/wiki/Visual_field
The video provides an example of a patient with a R visual field cut.. No sound
Abnormal CN V Sensory Exam
This patient demonstrates unilateral sensory dysfunction in the Trigeminal nerve. Recall that the the Trigeminal nerve is the primary nerve anesthetized during dental procedures.
Abnormal CN VII: Note the asymmetry in facial muscles
Abnormal CN XII (Hypoglossal)
The tongue will deviate toward the affected (weaker) side when the patient is prompted to stick out their tongue
Cranial nerve coordination examination
The VOR is also referred to as the "Doll's Eye's" reflex. The examiner (sound only) is assessing both eye motor function and coordination of eye and head motions which includes CN VIII
Examples of possible safety considerations for patients with CN deficits include:
This assessment is often individualized based on the contextual factors for the individual patient. Activities are closely aligned with the developmental sequence and home safety. Examples of functional assessments include (but are not limited to):
An initial assessment of gait includes
Coordination during gait may be included in the gait assessment. PTs and PTAs use observation and appropriate medical terminology to describe abnormal findings. Symmetry, synergies, endurance, and safety considerations may be included in the plan of care and should be reassessed to note progress toward goals and function.
Locomotion includes non-ambulatory mobility. Safety, endurance, requisite posture, and motor planning for maneuvering effectively at home and in the community are included in locomotion assessments.
Normal tandem gait
Abnormal gait examples
Neuropathic gait
Abnormal tandem
Parkinsonian gait
Ataxic gait
Diplegic gait - video is without sound
In each patient encounter, the PTA must think critically, engage diverse values and perspectives, create solutions, communicate effectively, apply learning to ensure skilled physical therapy services. Within each element of the patient encounter, a PTA uses analytical skills to recognize when changes or new data elements may indicate treatment is:
and communicates these findings (subjective and objective) with the supervising PT
The supervising PT analyzes all of the examination elements to develop a treatment prognosis and plan of care designed to progress the patient and meet treatment goals. A PTA must integrate evaluation findings and:
The role of the PT is to interpret the examination results, perform and/or delegate interventions in the plan of care, reexamine the patient as needed to assess response to PT, make changes to the treatment plan as needed, and consult with other health care personnel, including the PTA, as needed.
In addition to the essential role elements above, the following table summarizes the role of the PT and of the PTA in the examination and care planning process for patients with neurological dysfunctions:
|
Pt/Client Management |
PT |
PTA |
|
History |
Collects relevant history, consults multiple data sources, integrates knowledge of prior level of function (PLOF) and contextual factors (pathology, personal, environmental) into treatment approaches and planning |
Comprehend relevant history and it's impact on POC as indicated by supervising PT; collect relevant subsequent subjective and changes to condition Integrates information about patient's cognition, safety, and situation into subsequent treatment planning (e.g., communication and communication support, rest breaks, equipment, family/caregivers, coordinating treatment times with multidisciplinary team as indicated, etc.)
|
|
Body Systems |
Screen for conditions that indicate a need for referral to additional medical care providers; interpret systems review outcome and integrate information into prognosis and treatment plan |
Comprehend the general purpose and outcomes of a systems review (e.g., role of body systems in health maintenance, general knowledge of normal vs. abnormal responses, and "red flags"). Repeat relevant systems review with patient and compare results
|
|
Vital Signs and Pain |
Integrate findings into safety, frequency, intensity, prognosis, multidisciplinary care planning, and treatment |
Repeat prior and during treatment as indicated; recognize normal and abnormal findings; select and interpret standardized pain assessments Recognizes activities, positioning, and postures that aggravate or relieve pain or altered sensations
|
|
Observation |
Continuous process during patient encounter, includes posture, movement patterns and strategies, mental status, signs and symptoms of neurological involvement (e.g. gaze preference, limb neglect, etc.) |
Recognizes alignment of trunk and extremities at rest and during activities Recognize normal and abnormal movement patterns Recognizes and monitors responses to positional changes and activities Recognizes changes in the direction and magnitude of patient's state of arousal, mentation and cognition Recognizes activities, positioning and postures that aggravate or relieve pain or altered sensations, or that can produce associated skin trauma Distinguish language deficits versus memory deficits, so there is confidence in the accuracy of patient responses during assessment, activity tolerance, and consent to treat
|
|
Sensation |
Integrate outcomes of multimodal sensory assessment (exteroceptive, prioprioceptive, and combined cortical sensory function) into knowledge of condition and prognosis for return, recovery and/or adaptation (e.g., equipment, assistive devices and strategies) when forming the plan of care |
Repeat relevant sensory tests and measures and report outcomes (diminished, intact, absent) Recognize sensory patterns that increase risk of injury (skin, limbs, safety) Recognize deficits that correlate to specific movement impairments |
|
Motor |
Integrate analysis of multimodal motor assessment (tone, reflexes, righting reactions, coordination, movement patterns, and strength) into knowledge of body systems and resultant functional limitations |
Repeat relevant motor tests and measures and report outcomes Recognize the influence of neuromuscular tone on efficient and effective volitional movement Recognize movement patterns or deficits that increase risk of injury Recognize normal versus abnormal developmental reflexes and the resultant impact on progressing toward PT goals
|
|
Cranial Nerve Exam |
Screen for damage to peripheral nerves that originate from the brain; interpret impact on function |
Repeat relevant cranial nerve tests and measures and report outcomes Recognize abnormal vs.normal sensory and motor responses within cranial nerves Apply understanding of cranial nerve deficits when preparing for safe and effective treatment |
|
Balance |
Integrate analysis of posture, base of support, righting and protective reactions, and balance recovery strategies in static and dynamic situations; assess senorimotor functional as it relates to efficiently maintaining the center of gravity within a base of support |
Repeat relevant standardized assessments, test and measures and report outcomes Recognize normal versus abnormal righting reactions Apply understanding of limits of stability, equilibruim, strategies, and function to progress balance control as directed |
|
Functional Activities |
Integrate a combination of standardized and individualized functional assessments that are relevant to primary impairments and sensitive to changes; apply understanding of evidence to develop a prognosis and plan of care |
Repeat relevant standardized assessments, test and measures and report outcomes Interpret standardized outcomes as it relates to level of assistance, level of disability, fall risk, agility, etc. Select interventions as directed that are directly linked to minimizing impairments and resultant loss in function noted in plan and goals
|
|
Patient Participation |
Interpret patient report of impacts of impairments and functional limitation on ability to engage in individual life and community activities; apply understanding of evidence to develop a prognosis and plan of care
|
Employ approaches and techniques as indicated in the plan of care to optimize patient participation and mininimize participation restrictions in life and community |

