Abnormal Spine Curves
PTA 104 Orthopedic Dysfunctions
Introduction
Note: There are approximately 30 minutes of embedded screencasts and instructional videos as part of this interactive lecture.
One major pathological postural adaptation in the spine is scoliosis. In previous course work, we have learned the normal spinal curves and some common maladaptive postures with muscle length and strength imbalances. In this course page, we will go into more detail about the pathological processes which influence spinal curves
Note - I mentioned the "Unit 2" exam in the video - this is an error. This content is included in the Unit 1 exam
Objectives
- Define kyphosis, lordosis, and scoliosis
- Distinguish between normal and abnormal curves of the spine
- Describe causative factors of abnormal spinal posture throughout the life span
- Compare and contrast structural and non-structural abnormal curves
- Identify and describe methods of management and rehabilitation for kyphosis and scoliosis.
- Describe treatment interventions as it relates to degree of spinal curve
References
- Dutton, M. (2019). The Pediatric Orthopedic: In Orthopaedics for the Physical Therapist Assistant. 2nd ed., Jones & Bartlett Learning, Inc: Burlington, MA. p. 738-742
- Kaplan, S. L., Coulter, C., & Fetters, L. (2013). Physical therapy management of congenital muscular torticollis: an evidence-based clinical practice guideline: from the Section on Pediatrics of the American Physical Therapy Association. Pediatric Physical Therapy, 25(4), 348-394.
- Kisner, C., Colby, L.A. (Eds.) (2018) Therapeutic Exercise Foundations and Techniques. 7th ed., 2018, FA Davis: Philadelphia PA.
- Lombara, A., Callanen A. (2017). Congential Muscular Torticollis. CINAHL Rehabilitation Guide, EBSCO Publishing: Ipswich, MA. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=rrc&AN=T708612&site=rrc-live
Review of Spinal Alignment
Normal spinal alignment has been introduced in PTA 101 and reinforced in PTA 133L and PTA 104/104L
- Spine should be vertically straight
- Center of occiput should be aligned with center of sacrum
- Results in normal lordosis (cervical and lumbar curves) and kyphosis (thoracic and sacral curves)
- Postural abnormalities are identified primarily through observation; decreases or increases in spinal curves at rest are consistent abnormal postural findings
Scoliosis
Scoliosis is any lateral curvature of the cervical, thoracic, or lumbar spine; rotoscoliosis is an updated term that is more specific to the abnormal combined lateral curve with progressive rotation at individual spinal segments
Primary Onset of Scoliosis
- classified as idiopathic: infantile (0-3yr), juvenile (3-9 yr), adolescent (puberty to adult), or adult
- congenital - some correlation with family history
- idiopathic (cause unknown) is the most prevalent form
- 75%-85% of all recognized types of scoliosis
- idiopathic adolescent scoliosis comprises about 80% of scoliosis cases
- R thoracic is the most common
- neuromuscular causes, such as imbalances in tone, spasticity, or loss of muscle function (paresis and/or paralysis)
- degenerative disease
Associated Symptoms
- pain
- decreased cardiopulmonary function (usually with thoracic curves greater than 65 degrees)
- decreased digestive function
- neurological symptoms associated with spinal stenosis.
Sample scoliosis progression (Approximately 2 minutes)
Secondary Onset of Scoliosis
- osteoporosis
- trauma (e.g.,, fracture, leg length discrepancy)
Prognosis
- Prognosis is influenced by:
- age of onset - Younger age-onset is has a poorer prognosis
- type of curve - Double curves have a poorer prognosis than single curves
- degree of curve - the higher the degree, the greater expectations of comorbidities and functional changes. Severity is classified by degree of curve
- curve <= 25 degrees - monitor for changes
- curve 25 to <=40 degrees - use of orthotic; physical therapy is recommended
- curve > 40 degrees may result in surgical stabilization to prevent further progression
- gender - biological females have a 10 times greater risk for progression
Classifying Scoliosis
Recognized as either structural or nonstructural
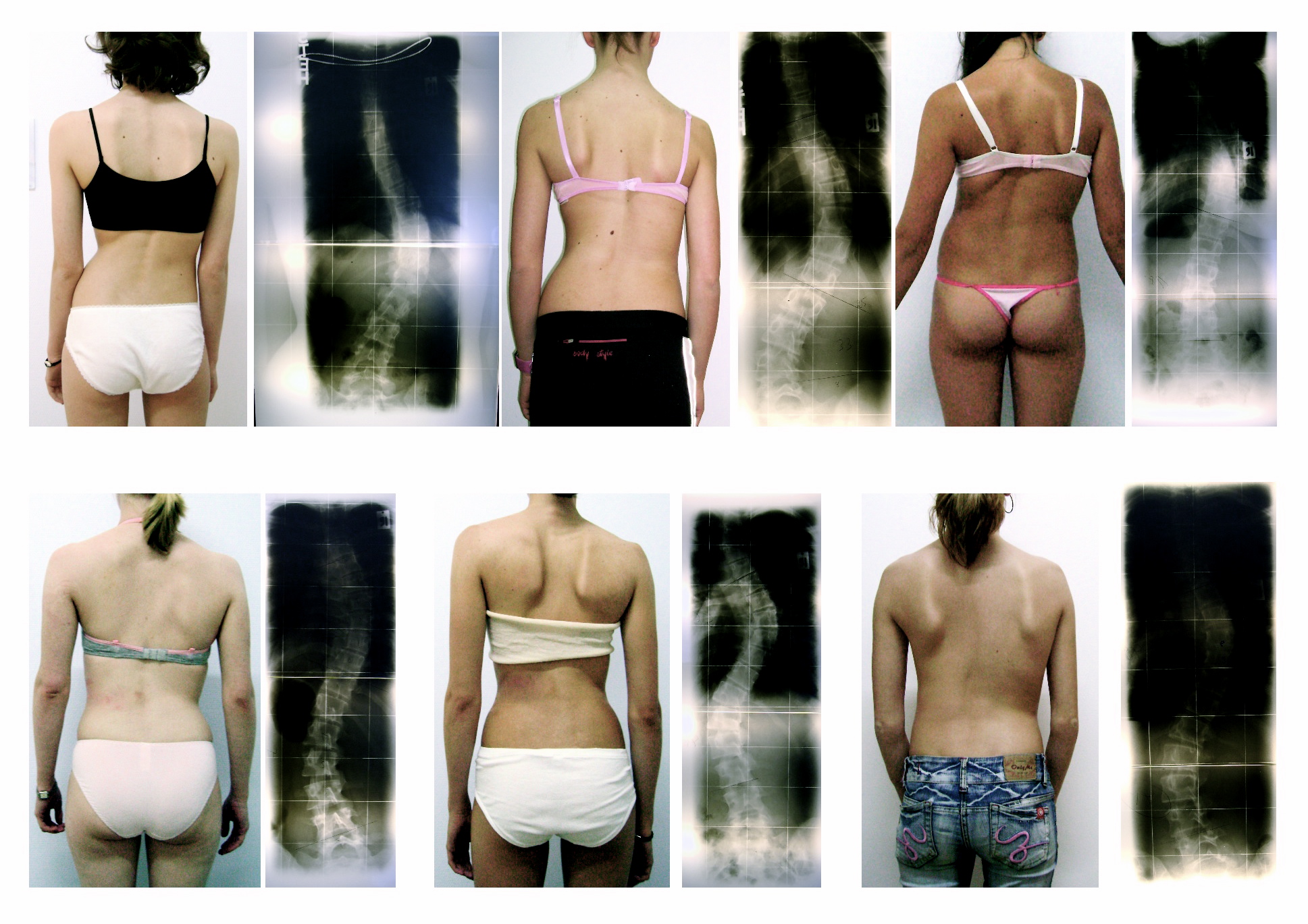
- structural: rotation of the spine is fixed, irreversible; lateral curves do not change with patient position or voluntary movement. The images below are examples of structural scoliosis
- non-structural: rotation of the spine is reversible; lateral curves are reduced with positional changes
Document observation findings to describe the scoliosis. Common documentation elements include:
- Side of the convexity: e.g. Right thoracic scoliosis
- Spine involvement: e.g., Right thoracic scoliosis
- Presence +Adams Forward Bend Test - rib hump during forward flexion indicates structural scoliosis named by side of convexity - direction of rotation
- Number of rotation curves - single vs. double
Interventions for Scoliosis
Conservative
- Focus is on improving spinal motion, increase muscle strength, and reducing back pain
- Typically involves
- strengthening of all muscles on the convex side
- facilitated manual stabilization
- contract relax techniques
- proprioceptive training
- progressive against gravity
- stretching of all muscles on the concave side
- prone reaching
- sidelying gravity-assisted
- quadruped rock with reach
- axial elongation stretching
- Abdominal strengthening
- Spinal extension strengthening
- Bracing: Milwaukee Orthosis as an example
- Breathing
- Endurance training - aquatics
Demonstration Video (Approximately 2 minutes)
Demonstration Video (Approximately 3.5 minutes)
Surgical
- Typically indicated for spinal curves greater than 40 or more degrees
- Involves placement of rods along the spine to resist further rotation
Other Abnormal Spine Curves
Kyphosis
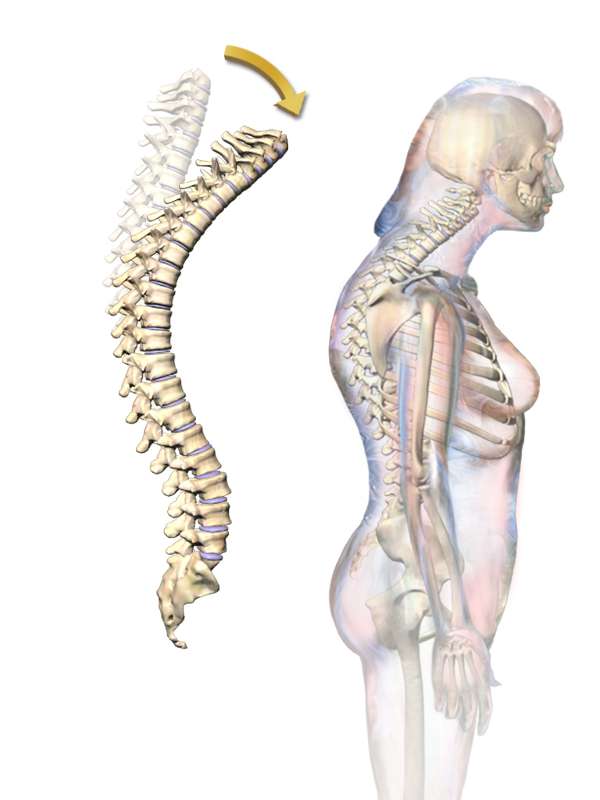
By BruceBlaus [CC BY-SA 4.0 (https://creativecommons.org/licenses/by-sa/4.0)], from Wikimedia Commons
- A rounded back posture (and protracted scapulae)
- Associated with osteoporosis and history of multilevel compression fracture; more severe deformities are generally idiopathic
- Exercise intervention principles are similar to scoliosis
- Strengthen muscles on the convex (lengthened side): spinal extensors and scapular retractors
- Stretch muscles on the concave (shortened side): scapular protractors and spinal flexors
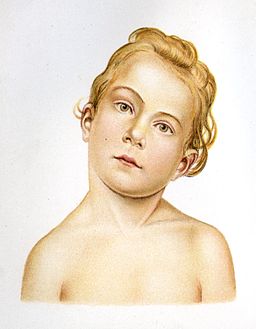
Congenital Torticollis
- Cervical spinal curve characterized by contracture of the SCM musculature
- Characteristics include lateral flexion the same side as the contracture, rotation toward the opposite side, and facial asymmetries
- Etiology is unknown; pediatric screening around 2 days old for any limitations in cervical range of motion or emerging facial asymmetries. Diagnosis is typically made around 3 weeks of age
- Contributing factors:
- Malposition in utero
- Breech position in utero
- Birth trauma: traction to spinal nerve roots resulting in SCM palsy
- Clinical practice guidelines for physical therapy include:
- PT infant assessment of posture, ROM, pain behaviors, skin integrity, and craniofacial asymmetry. If cranial shape is a contributing, factor, the infant may be fitted with a custom cranial remodeling orthosis
 https://www.flickr.com/photos/150hp/6271381480/in/photostream/
https://www.flickr.com/photos/150hp/6271381480/in/photostream/
- neck PROM, trunk and neck AROM, symmetrical movement development
- KEY POINT: Family and caregiver education is critical. Parents should be given activities that promote opposing cervical motion, such as positioning, games, stretches, and positioning
- Children over the age of one may be eligible for surgical release of SCM if there has been limited response to conservative treatment
 http://upload.wikimedia.org/wikipedia/commons/5/53/Siebert_22_-_Torticolis.jpg
http://upload.wikimedia.org/wikipedia/commons/5/53/Siebert_22_-_Torticolis.jpg
Role of the PTA
In addition to interventions to minimize the affects of scoliosis on movement and function, PTAs are qualified and may engage in wellness screenings, such as postural scoliosis screening.
PTAs have knowledge of standard bony landmarks and are qualified to observe abnormalities in symmetry at the pelvis, trunk, scapula, head and shoulders from multiple angles.
Screens are not diagnostic. Screen outcomes are used to facilitate appropriate referrals for evaluation and treatment
Approximately 4 minute video
End of Lesson
Be prepared to apply your understanding of spine curves to selecting movement-based interventions.