Spinal Disorders
PTA 104 Orthopedic Dysfunctions
Spine Conditions - Instructional Use Statement
The following information is used for instructional purposes for students enrolled in the Physical Therapist Assistant Program at Lane Community College. It is not intended for commercial use or distribution or commercial purposes. It is not intended to serve as medical advice or treatment. Contact howardc@lanecc.edu for permissions.
Introduction
In this lesson, students will apply knowledge of anatomy and kinesiology of the spine to specific disorders encountered in physical therapy. The content and instruction assumes students have a working knowledge of the bones, ligaments, nerves, and muscles of the spine. Spinal pain is the number one reason people encounter and use physical therapy. PTAs must have an understanding of normal and abnormal spinal function and degenerative conditions in order to correctly select, apply, and compare results with the physical therapy evaluation and assessment.
Objectives
- Identify major function and motions of the cervical, thoracic, and lumbar spine
- Describe common characteristics of healing phases for spine conditions
- Describe factors that contribute to common spine conditions:
- presentation (signs and symptoms)
- commonly involved spinal segments where relevant
- causes and/or prevention (e.g. structures and/or motions, muscle imbalances)
- co morbidities and psychosocial contributors
- Differentiate between conditions of hypomobility versus instability
- Discriminate between clinical scenarios which indicate a surgical or other medical emergency/complication
- Compare and describe common spine surgeries
- Describe findings of musculoskeletal, neuromuscular, and special tests performed during PT examination of spinal disorders.
- Compare and contrast classification systems for low back and spinal pain
Spine Function and Motion
The purpose of the spine is to:
- provide structural stability
- protect the spinal cord and spinal nerve roots
- allow static postural control in weight bearing for sustained periods
- contribute to functional gait.
In most cases, functional recovery from a spine condition that is painful interferes with function is described by three phases: acute, subacute, and chronic.
6 minute video
Structure Reminders
Students are expected to recall specific structural elements, including landmarks, range of motion, joint function, ligaments, and the names of stabilizing and mobilizing muscles from PTA 132 and PTA 132L. Students are expected to recall spine motions that increase or decrease the foramen in a spine segment.
In general, ligaments function to resist excessive spine motion, especially in flexion and extension. Although facet joints are all designed to be load-bearing, these joints change in shape and function depending on their location (e.g., cervical, thoracic, and lumbar), allowing motion in some cases and restricting motion in others.
Neck conditions refer to symptom presentation between the occiput and T3; back conditions refer to symptom presentation inferior to 12th rib to the gluteal folds.
The sacroiliac joint (SI) is related to lumbar spine conditions due to the amount of forces that occur at the lumbosacral junction with loading and weight bearing. The SI joint has structural (e.g. bony, ligamentous, thoracolumbar fascia) components that provide significant stability and dynamic stabilizers that are engaged during movement (e.g. latissumus dorsi, gluteals, abdominals, biceps femoris, adductors). Knowledge of ligaments and muscle origin and insertion in the lumbopelvic region is essential for treating low back pain and for general spinal stabilization and conditioning interventions.
Healing Stage Characteristics
There are three (3) general healing stages that guide clinical-decision making in managing spine conditions. These "healing" stages can be applied based on symptom presentation in non-specific and specific spine conditions:
Healing Stages
|
Acute - "Protect"
|
Subacute - "Controlled Motion"
|
Chronic - "Return/Optimize Function"
|
|
Reduce pain
Reduce inflammation
Short term use of biophysical agents, heat/cold
Apply orthoses as needed
|
Initiate exercises to address muscle imbalance
Stabilization of flexors/extensors; scapula and lumbopelvic area
|
Progress functional activity training such as lifting, carrying, and reconditioning
|
|
Decrease joint load
|
Initiate postural training
Caution with activities and postures in end-ranges
|
Integrate neuromuscular control principles to prevent recurrence
|
|
Initiate aerobic conditioning
|
Progress aerobic conditioning
|
Sustain aerobic conditioning as a long-term routine
|
|
Advance ROM in non-provoking (e.g., pain-free) directions, initially in non-weightbearing positions
Submaximal isometric strengthening
|
Advance ROM in partial and full weight bearing positions
|
Progress active and resistive exercise for recovering function, including combined (e.g., multiplane) motions
|
In a longitudinal study, patients who initiated a physical therapy plan of care for a new onset of low back pain management were much less likely to use opioids for short-term and long-term pain management
According to the National Institute of Health, low back pain is experienced by 80% of adults and is the most frequent reason for referral to physical therapy. However, in a recent longitudinal study, only 10% of patients who saw a doctor because of low back pain were prescribed physical therapy.
Spine Conditions
The following provides an overview of signs and symptoms primarily associated with cervical and lumbar conditions
12 minute video
Radiculopathy
- Spinal nerve / nerve root conduction is impeded due to "encroachment into peripheral nerve tissue spaces resulting in nerve compression or ischemia";
- encroachment can be classified as direct or indirect, mechanical or chemical
- direct - mechanical : direct compression pressures from structures or motions is place on spinal nerve(s)
- indirect - mechanical: blood flow decreases (ischemia) to the spinal nerve from direct pressure (compression or stretch) or from scar tissue formation around nerve tissue
- direct - chemical: nuclear material from herniated intervertebral discs encroaches space
- indirect - chemical: ongoing cellular inflammatory responses with tissue edema
- Compression can be due to stenosis in the central canal or foramen by bony and/soft tissue changes, tumor, or disc bulge/herniation
- Associated signs and symptoms: Numbness (sensory n.), weakness (motor n.), muscle atrophy, impaired deep tendon reflexes, sensory changes in affected nerve root distribution
Sciatica
Sciatica is a radicular condition associated with pain in the low back and lower quarter,specifically pain that extends down the posterior lower leg, including the foot. It is typically unilateral, but can present bilaterally. It is most commonly caused by intervertebral disc herniation, and is also associated with degeneration, infection, stenosis, and pelvic instability. Patient who have increase pressure on the sciatic nerve due to pregnancy, posterior hip/buttock trauma, or inflammation of the piriformis muscle may also report sciatica symptoms
- sharp, dull, burning or radiating pain often associated with numbness and parasthesias
- may include weakness and loss of reflexes
- L4: patellar reflex, medial sensation
- L5: dorsiflexion, lateral sensation
- S1: Achilles reflex, plantar flexion, posterior sensation
- aggravated by coughing, sneezing, valsalva
- movement is generally guarded and stiff, especially in the trunk and affected hip
- Cauda Equina Syndrome: considered a surgical emergency
- sudden change in bowel/bladder function (urinary retention, loss of sphincter control) or
- sudden loss of sensation in the perineum ("saddle anesthesia")
- bilateral sciatica symptoms
- treatment is typically conservative with PT x 6-12 weeks with follow-up MRI/CT if there is no improvement; epidural steroid injections can be helpful for symptom reduction.
Intervertebral Disc Conditions
Although disc herniation can result in pressure on the nervous system tissue, either from direct contact or from chemical irritants from inflammation, a majority of these cases resolve over time with conservative treatment. The evidence for long-term relief with surgery is mixed, with exceptions for situations that markedly reduce strength and sensation.
- Disc structure allows for distribution of force during weight bearing through the spine during static posture and during spine motions in multiple planes
- Foraminal disc herniations are the most symptomatic
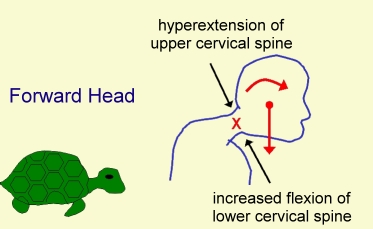
- Degenerative changes increase in the cervical spine with postural imbalances, primarily forward head
- Degenerative changes increase in the lumbar spine with repetitive compression (e.g. heavy lifting in flexion) or trauma (e.g. fall); degenerative changes may be asymptomatic
- Nucleus pulposus desiccates over time, decreasing its ability to absorb and distribute weight bearing and rotational forces; age-related change; disc rehydration occurs during sleep and recumbent positions Increased calcification, fracture risk, and decreased density at vertebral end-plates The affected nerve root is between spinal levels (e.g. C5-6 involves C5 nerve root)
- Annulus fibrosis can tear, resulting in decreased resistance to torque and increased risk of extrusion of disc contents; risk of herniation of nucleus pulposus increases with annular tears
- Annular tears usually occur posteriorly where the annulus is weakest; herniation may be central, posterior, or posterior-lateral (e.g. foramen).
- Discs may bulge without evidence of annular tearing or herniation
- Most common site of disc herniation is
- C5-6
- C6-7
- L4-5
- L5-S1
- in the cervical spine, the greatest amount of flexion motion occurs at C5-6
- in the lumbar spine, the lower segments are more vulnerable because the posterior longitudinal ligament ends at L3.
Spinal Stenosis
Stenosis refers to a narrowing in the central canal or associated spinal foramen due to degeneration of bony structures and ligaments. Space within the canal/foramen changes with spinal motions:
- flexion --> central canal widens
- extension --> central canal narrows
Cervical signs and symptoms->decreased strength and dexterity in hand, decreased grip function, pain, numbness in hands, potentially impaired balance/gait
Lumbar signs and symptoms -> pain (affected side or bilateral), numbness and LE weakness
Neurogenic claudication describes pain that results from ischemic compression on the nerve root, producing signs and symptoms in the legs with prolonged standing/extension and is relieved with lying down or sitting (flexion). There is increased pain with walking down inclines due to increased lumbar extension
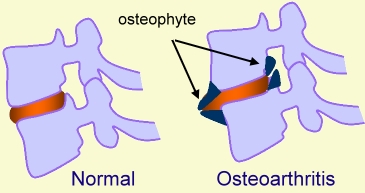
Osteoarthosis
- usually appear at the uncovertebral and/or facet joints
- osteophytes are one of the space-occupying lesions which may lead to radiculopathy
- spondylosis is used to describe osteoarthosis in the spine at the margins of the vertebral bodies
Facet Joint Pathology
Facet joint pathology is a type of osteoarthrosis in the spine. It is a degeneration at the facets that results in bone spurring or related changes to bone tissue. Symptoms include:
- painful restricted motion
- in the cervical spine, pain is typically provoked with combined motions of extension, side bending and rotation
- achiness which may radiate into the shoulder (cervical) or lower leg (lumbar)
- complaints of the lumbar area clicking, locking or "going out"
Spondylolysis and Spondylolisthesis
Spondylolysis
Fracture of the pars interarticularis (segment of bone between the superior and inferior articulating facets)
In the image below, notice how the spinous process has separated from the lamina. Result is instability at the affected segment and abnormal weight-bearing forces in adjacent spinal segments. You should notice how the vertebra translates forward in the sagittal plane with respect to adjacent vertebra. This can occur with repetitive forces and due to some forceful impact in extension, such as hopping and landing on one foot with force
Spondylolisthesis
Mostly a condition of the lumbar spine which is associated with chronic, repetitive trauma. Instability of longitudinal ligaments from repetitive force or excessive motion causes the segment to move anteriorly or posteriorly. Anterolisthesis is most common and may require surgical fusion to prevent further instability or loss of nerve function.
Ankylosing Spondylitis
An inflammatory condition of unknown etiology which initiates as inflammation in the sacral region. It results in progressive loss of spinal motion due to progressive inflammation and vertebral fusion.
Whiplash-Associated Disorders (WAD)
Refers to bony and/or soft tissue injury in the cervical spine and upper quarter due to acceleration-deceleration forces. Injury is to ligaments and muscles; stretch forces to neuromuscular structures may account for increased sensitization. Due to complaints of dizziness and balance changes, these patients may be a fall risk.
Outcomes for WAD are negatively affected by fear avoidance or catastrophizing behaviors. Examples include patient belief that the symptoms will never improve.
Symptoms of WAD include:
- pain
- headache
- decreased spinal mobility
- stiffness
- low back pain
- shoulder pain
- visual disturbances
- dizziness
Classification of WAD
- Grade 0: No pain or physical symptoms
- Grade I: No physical signs of musculoskeletal dysfunction; subjective reports of pain, stiffness, and tenderness
- Grade II: Some physical signs of cervical movement dysfunction; subjective symptoms reported
- Grade III: Physical and neurological signs of cervical dysfunction; subjective symptoms reported
- Grade IV: Pain with fracture or dislocation
Sacroiliac Dysfunction
This is characterized by non-specific low back and hip pain, which may radiate into the groin. Other symptoms include sharp pain with position changes in bed, point tenderness in PSIS or pubis, pain with stairs, sit to stand, or hopping on one leg. Pain may also be provoked in end-range straight leg raise
Instability may result from trauma or overuse, and may involve the ligaments or be driven by muscle imbalances that place rotational or translational forces through the joint. Muscle length tension contributors include hip flexors, hamstrings, gluteals, erector spinae, quadratus lumborum, and abdominals
Self-Assessment
Prepare for the test by checking your understanding of spine conditions in the lecture.
Common Spine Surgery
- Foraminotomy: Bone and/or other fibrous tissue is removed in and around the foramen to decompress the affected nerve root
- Laminectomy: The vertebral lamina is removed to decompress the central canal or to relieve pressure secondary to spondylosis and spondylolisthesis
- Discectomy: A portion of the herniated disc is removed to decompress nervous tissue; involves a laminectomy to access disc contents
- Fusion: Use of hardware, bone grafts, screws and metal cages to eliminate segmental motion due to instability and/or pain
- Disc replacement: replacement of IVD with prosthesis
- Vertebroplasty: bone is injected with cement-like compound to increase strength of bone tissue following compression fracture
Post-operative Complications
- thrombophlebitis
- pulmonary infection
- hardware failure
- persistent pain
- sexual dysfunction
- spinal cord injury
- pseudoarthosis
PT Examination and Evaluation
History: Includes positions and movements which increase and/or relieve pain, duration of symptoms, level of irritability, pattern during the day/night, pain quality and location, onset and history of previous episodes.
May include self-report questionnaires to quantify level of pain and/or disability due to lumbar symptoms; can be used to differentiate between physical findings and psychosocial contributors to pain presentation.
Red Flags
During the examination, the PT will review the patient's history to rule out evidence of serious medical pathology. PTs use a systems review process to confirm the condition is within the scope of practice of physical therapy:
- Violent trauma
- Constant, progressive pain that does not change with movement or position
- Thoracic pain
- history of carcinoma, steroid use, drug abuse
- HIV
- Unexplained weight loss
- Persistent severe restriction of lumbar flexion
- Widespread neurological symptoms
- Structural deformity
Musculoskeletal
7 minute video
2 minute video
- postural deviations may indicate mobility restrictions (joint, muscle, etc)
- PTs may assess a patient's ability to self-correct postural deviations with verbal and/or tactile cues
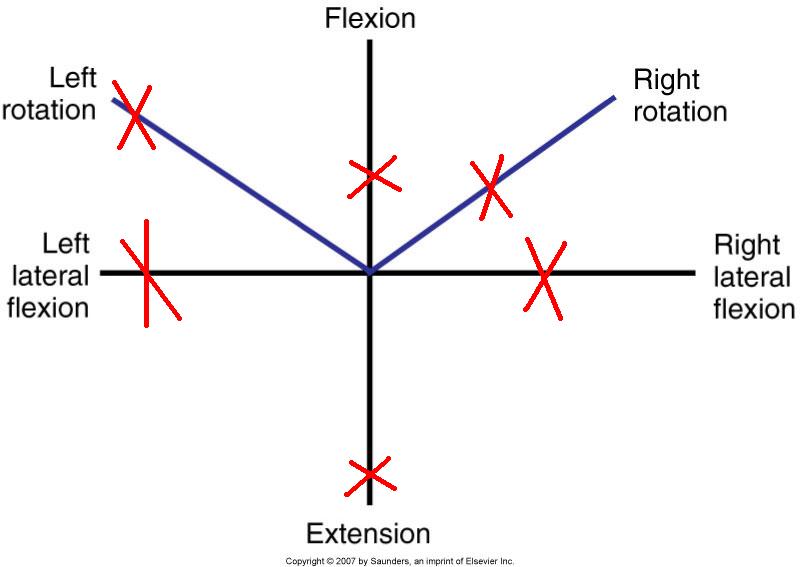
- Range of motion is the primary impairment in LBP and is used to evaluate response to treatment. PTs may use a visual scale to document AROM as it relates to normal values. PTAs consult the evaluation for visual or quantitative assessment of spinal ROM
- ROM includes assessing response to overpressures when AROM and repeated AROM are pain-free or minimally symptomatic. The PT will apply gradual manual force to the spine in its end-range to provoke or clear symptoms with each spinal motion or with combined spinal motions (e.g., flexion + rotation R)
- Accessory segmental spinal motion is assessed and is classified as normal, hypomobile, or hypermobile
- abbreviated as PPIVM (passive physiological intervertebral mobility)
- hypomobile: benefits from mobilization, manipulation, stretching and stretching of related muscles
- hypermobile: benefits from stabilization
- Muscle length: often coincides with ROM testing; includes length of muscles which originate or insert on the spine/pelvis
- Muscle strength: MMT and functional tests are used to determine nerve root involvement and may provide information on secondary muscle guarding influences due to pain/perception of pain
- Mechanical Provocation Tests
7 minute video
- used by the PT to determine motions and involved structures which reproduce patient's primary complaint
- Quadrant/Foraminal closure test
- Spurlings is a combination of cervical SB + extension + axial compression + overpressure
- Positive (+) Spurlings is an indicator of cervical intervertebral disc or foramen dysfunction (radiculopathy)
- Cervical Compression
- Pressure is applied through the top of the head (axial loading)
- Positive (+) cervical compression is an indicator of nerve root impingement
- Cervical Distraction
- Cephalad manual traction is applied through the occiput
- Positive (+) cervical distraction test is reported when patient's symptoms decrease during traction and indicates cervical radiculopathy
Neuromuscular
- Pain: PT palpates painful and related structures, noting for warmth and tissue reactivity
- Peripheral nerve integrity: assessed through sensation testing and MMT for spinal dermatomes and myotomes respectively
- Reflex integrity: DTRs which are exaggerated, diminished or absent indicate spinal or other nervous system pathology
- Neurodynamic tests: Involves applying mechanical stress (stretch) to nervous tissue to distinguish nerve root compression and peripheral neuropathy contributors to patient's complaint
- Straight leg raise (SLR): Positive (+) indicates involvement of lumbosacral nerve roots. The PT should note the degrees of hip flexion when symptoms are elicited. Symptoms can present unilaterally, contralaterally or bilaterally. The PT may include medial hip rotation, hip adduction, ankle dorsiflexion, and/or cervical flexion to increase tension on nerve tissue.
- Prone knee flexion: Positive (+) indicates L2 and/or L3 involvement; may also produce SI pain due to restrictions in the rectus femoris
- Slump test: Positive (+) indicates lumbosacral nerve root compression or lumbosacral nerve involvement
- Upper Limb Tension Test (ULTT): Positive (+) indicates involvement of nerves in the brachial plexus. Movement tests are specific to radial, ulnar and median nerves
Special Tests
- Vertebral artery test: Positive (+) indicates evidence of vertebral artery compromise with end-range cervical motions, especially rotation and extension. High velocity joint manipulation or end-range motions are contraindicated
- SI Joint tests
- Abnormal SI mobility is classified as sacroiliac (abnormal positioning of sacrum on a normally positioned ilium) or iliosacral (abnormal positioning of the ilium on a normally positioned sacrum)
- Standing flexion test: Positive (+) if the PSIS moves upward (cephalad) and forward during lumbar flexion with respect to the contralateral side. Indicates restricted mobility of ilium on sacrum (iliosacral problem)

Sacral fixation test/Gillet's Test: Positive (+) if there is no PSIS movement as one hip flexes toward the trunk (iliosacral problem) (Approximately 1 minute)
Sitting flexion test: Positive (+) if PSIS moves cranially as trunk flexes forward (iliosacral hypomobility) (Approximately 30 seconds)
- Long sitting test: Used to determine abnormal rotation of the innominate on the sacrum
- moving from supine to long sit --> limb appears to lengthen in long sitting--> indicates posterior innominate rotation
- moving from supine to long sit --> limb appears to shorten in long sitting --> indicates anterior innominate rotation
- Compression tests: Positive (+) if manual compressive forces applied in supine to the SI joint(s) reproduce pain complaint
- Limb length inequality: Positive (+) if observed asymmetries with bony landmarks can be minimized or eliminated with placing blocks or shims under the shorter limb
- Prone instability test: Positive (+) if low back pain is reproduced with joint mobilization during active recruitment of lumbar extensors
- Thomas test: Positive (+) if hip flexion is greater than 0 degrees when controlled for lumbar extension. Indicates decreased mobility of hip flexors

Demonstration of Cervical Stabilization Progression
6 minute video
Classification Systems for Spinal Disorders
A key point with classification systems is that they are used by physical therapists as a framework to guide clinical-decisions. Following an examination, a physical therapist may use a classification (e.g., "Flexion-Bias" or "Postural Syndrome" to identify a PT diagnosis that guides treatment
McKenzie Method
Most common classification system for low back pain used in physical therapy
Patients are classified as having mechanical pain (reproduced with movement) or non-mechanical (associated with inflammation or other pathology)
Results of PT examination leads toward categorization of mechanical low back pain. Patients with neuromuscular findings are generally not included in a McKenzie classification system
Specific elements of the PT examination include:
- history
- posture
- movement testing (standing, sitting, prone, prone, etc.); repeated and sustained movements/positions
- pain with movement
- palpation and joint mobility
- range of motion
Movement testing
Lumbar motion tests are performed in straight planes and with combined motions
The PT monitors symptom location and intensity with sustained and repeated motions
centralization: pain presents proximally and in the spine
peripheralization: pain presents proximally and radiates laterally and distally with movement
Following the examination, patients are can be placed in one of three (3) syndromes:
- Postural
- Dysfunction
- Derangement
Treatment-Based Classification
Determines if the patient can be managed by PT alone or requires MD or other health care provider involvement. Delitto using descriptions to classify intervention approaches for the spine based on what reduces symptoms and is most likely to allow progression. Using Delitto's system, spine conditions are classified as needing: (1) immobilization, (2) mobilization, (3) specific exercises, or (4) traction.
In general, treatment-based classifications use directional preference for movement and symptom modulation as a way to develop interventions to restore function.
Movement-Based Impairment (Sahrmann)
This system assesses postural and spinal changes in static positions and with limb motion in a variety of positions. Patients are classified based on the direction of motion which reproduces the pain complaint and compensatory strategies. Treatment emphasis is on restoring normal muscle length/balance and eliminating compensatory strategies.
End of Lesson
In lab we will apply some of these concepts to exercise selection and traction applications.
I recommend you work through the practice activities more than once to confirm your understanding of the material as it relates to the objectives