
Exercise and ADL Interventions for the Hip
104L Orthopedic Dysfunctions Lab
The following should be a review of kinesiology from PTA 132. Please take some time to review normal and abnormal gait including ROM at the hip and pelvis for gait.
Pelvic motion in frontal and transverse planes is named by what occurs at the unsupported side of the pelvis
|
Trunk Muscles |
Hip Muscles |
Pelvic Motion |
|
Trunk Extensors |
Flexors |
Anterior tilt |
|
Trunk Flexors |
Extensors |
Posterior tilt |
|
|
Abductors |
Caudal lateral tilt (hip drop) |
|
Ipsilateral flexors |
Adductors |
Cephalad lateral tilt (hip hike) |
|
|
External Rotation |
Forward rotation |
|
|
Internal Rotation |
Backward rotation |
Hip and pelvic motion influences stresses and repetitive strain to the lumbar spine and knee. The physical therapist will often screen the joints above and below symptoms in order to determine how limitations and/or instabilities may contribute to painful symptoms or other subjective and objective limitations.
PTAs should be able to identify and describe the influences of decreased flexibility on hip and pelvis motion so that patients may understand why specific stretches in their home exercise program may be helpful in progressing the patient toward their goals. Patients with postural impairments, asymmetries and movement dysfunctions will benefit from clear education in the effects of decreased tissue mobility on function.
Inadequate recruitment of the gluteus medius, inadequate recruitment of the iliopsoas, decreased mobility of the IT band, TFL and gluteus maximus, and over recruitment of the TFL, hamstrings, and lateral trunk flexors can impact motion throughout the kinetic chain. The PT examination will provide results of tests and measures that assess the length-tension and strength relationships on function. A PTA should be able to read the PT evaluation and comprehend the goals regarding strengthening, lengthening, and stabilizing involved segments. Knowledge of postural impairments allow the PTA to education on injury (and reinjury) management and prevention.
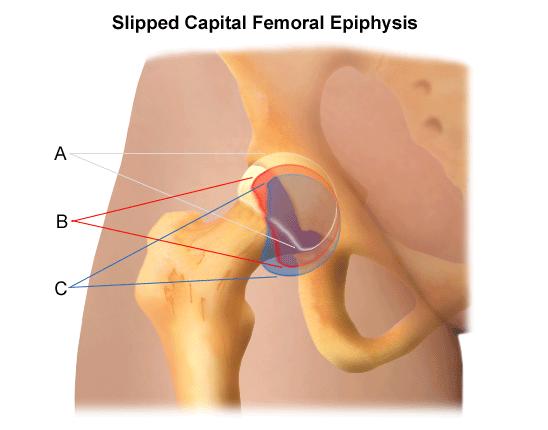
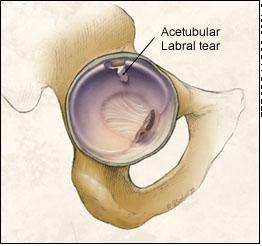
Pathologies at the hip have the greatest impact in weight bearing activities. Pain, restricted motion and abnormal posture lead to abnormal gait, balance dysfunction, and repetitive motion injuries
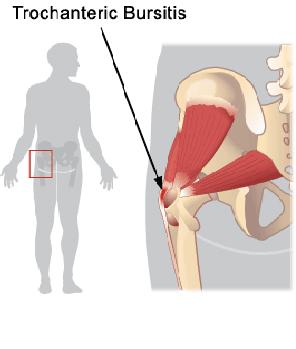
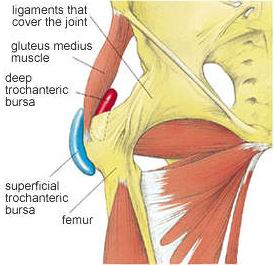 Notice the structures which influences stresses to the trochanteric bursae. Symptoms consistent with greater trochanteric pain syndrome (previously called "trochanteric bursitis", can benefit from interventions (exercise, joint protection, physical agents, etc.) for soft tissue pathology. Stretching and strengthening of associated structures can prevent recurrence of condition.
Notice the structures which influences stresses to the trochanteric bursae. Symptoms consistent with greater trochanteric pain syndrome (previously called "trochanteric bursitis", can benefit from interventions (exercise, joint protection, physical agents, etc.) for soft tissue pathology. Stretching and strengthening of associated structures can prevent recurrence of condition.
Your lab packet has a pre-lab worksheet that extends your knowledge from PTA 132L and asks you integrate observation, knowledge of conditions, and possible modifications into your thinking. Be sure to complete the pre-lab packet and bring it to lab.
Last term, you applied kinesiology when selecting a basic, intermediate, and advanced exercise for the lower extremity. PNF for the lower extremity was introduced as an intervention to progress ROM into resistance using manual contact and verbal cues to facilitate a response.
Warm-up exercises should preceed any resistance exercise. Consider stretching prior to resistance training to optimize ROM while training. Resistive training is specific to the patient population. This includes age, comorbidities and surgical considerations. Here are some general age-specific recommendations for resistance training. A summary of major concepts is included below:
|
Healthy Adults |
Children (6+) |
Older Adults (65+) |
|
Move through full, available, pain-free range |
Close, continuous supervision; ergonomics suited for child |
Close supervision and medical clearance to participate; monitor vital signs |
|
Include both concentric and eccentric |
Light weights (1-2#) |
Low resistance, low repetition; care with eccentric activities to minimize joint strain |
|
At least 8-12 repetitions of moderate intensity; 1-3 sets, 2-3 times a week |
At least 8-12 to 12-15 repetitions with emphasis on multijoint motions; 1-2 sets, 2 times a week. |
At least 10-12 repetitions at low to moderate intensity x 6-8 weeks before progressing; 2-3 x week with 48 hrs rest in between |
|
Slow to moderate speeds of motion; 2-3 minute rest intervals |
Low intensity, short duration, play-themed activities; 3 minutes rest during resistance intervals |
Movements should optimize joint protection; avoid high resistance in end-range; |
|
Gradual increase in intensity for progressive strengthening |
Increase intensity by increasing repetitions first, then increasing resistance by small increments |
Increase intensity by increasing repetitions first, then increasing resistance by small increments |
|
|
|
Modify or avoid exercises that strain or reinforce age-related postural changes |
|
|
|
Consider strengthening in sitting to decrease risk of LOB |
Plyometrics train muscles to rapidly produce force and quickly accelerate and decelerate in multiple planes of motion. A high degree of trunk control, soft tissue mobility, and dexterity is required to safely and effectively perform these exercises.
There are some examples of these advanced techniques in some of the linked web resources below.
Exercise prescription considers surgical and individual precautions and contraindications; skilled exercise instruction includes observing,and correcting compensation for under and over recruitment of synergists. Failure to provide adequate feedback, correction, and progression according to tissue healing parameters and surgical guidelines can result in repetitive strain to neighboring joints, soft tissue overuse syndromes, or surgical failure.
PTAs use their eyes and hands to monitor for a patient's ability to perform exercises correctly and safely within the parameters of their pathological conditions and comorbitities. PTAs understand considerations for progressing a patient safely toward rehabilitation goals.
Set up and safely apply exercises with elastic tubing or bands to strengthen major muscle groups of the upper and lower extremities. Include a dynamic open-chain, a dynamic closed-chain (if possible), and an isometric exercise for each muscle group.
|
Hip joint |
Open Chain |
Closed Chain |
Isometric |
|
Hip flexors |
|
|
|
|
Hip extensors |
|
|
|
|
Hip abductors |
|
|
|
|
Hip adductors |
|
|
|
|
Hip internal rotators |
|
|
|
|
Hip external rotators |
|
|
|
Now: Consider a patient who has the following restriction:
How will you modify the home exercise program for each condition?
What soft tissues are involved, and how can you use manual therapy (soft tissue mobilization) to help decrease pain and improve muscle performance?
Be prepared to answer these questions in lab
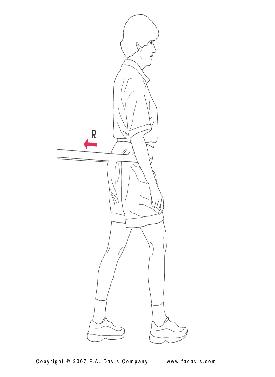
Resisted walking with theraband at pelvis can progressively increase recruitment of hip and core muscle for stable gait. In addition to marching and forward/backward gait, you can challenge lateral stability by walking away from the anchor at a diagonal.

Surgical precautions or chronic joint limitations can signficantly limit functional mobility, independence with self-care, and gait. Occupational therapy is an excellent resource for patients who may benefit from training in adaptive techniques for dressing.
We will have an opportunity to practice with ADL equipment commonly prescribed post-THA or hip ORIF in lab.