Locomotion Training
204L Neurological Dysfunctions Lab
Instructional Use Statement
The following information is used for instructional purposes for students enrolled in the Physical Therapist Assistant Program at Lane Community College. It is not intended for commercial use or distribution or commercial purposes. It is not intended to serve as medical advice or treatment.
Contact howardc@lanecc.edu for permissions
Key Concepts for Locomotion:
- Neuromuscular reeducation principles are both task-oriented and based in developmental positions and progressions.
- Developmental activities are sequenced to allow maximum function within the ability of the patient
- Coordination, strength, flexibility, and balance are treated in the context of performing a facilitated or independent developmental activity
- Progressions are typically sequenced according to the following pathway:
- mobility: can the patient initiate the movement into the position?
- stability: can the patient maintain the position against gravity?
- dynamic stability: can the patient perform weight shifts and movements in the developmental position?
- skill: can the patient do all of the above efficiently and effectively while engaged in an individualized functional activity?
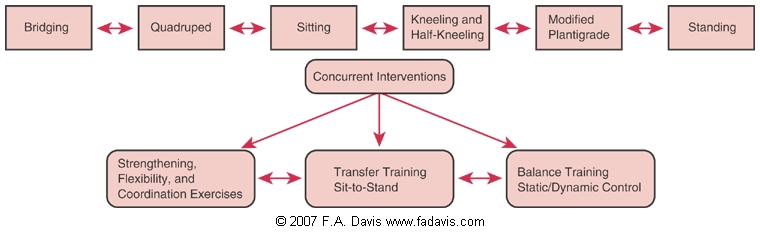
Preparatory Exercises for Locomotion Training
Bridging
Quadruped
- allows weight bearing through multiple joints
- inhibits spasticity in quadriceps and finger flexors
- rocking and weight shifting can be used to increase ROM, decrease spasticity, and increase trunk endurance in trunk and cervical extensors
- modifications and progressions:
- quadriped over ball/bolster: allows for partial weight-bearing in trunk
 http://www.whcenter.org/body.cfm?id=556940
http://www.whcenter.org/body.cfm?id=556940
- reaching in quadriped creeping
- functional activity: fall recovery and floor to stand requires motor control and planning from quadriped position
 https://www.hep2go.com/exercise_editor.php?exId=342&userRef=okqdclggnism
https://www.hep2go.com/exercise_editor.php?exId=342&userRef=okqdclggnism
Test question
Sitting
- short sitting: hips and knees are flexed with feet flat on floor
- long sitting: hips are flexed and knees are extended on supporting surface( dependent on hamstring length)
- includes weight shifting and scooting in sitting, with and without UE support
- progressions
- feet unsupported
- unstable surface (gym ball, balance disc/board)
- seated push ups are functional activities for SCI/tetraplegia conditions
- therapy balls can increase proprioceptive input and dynamic control on the involved side.
 http://www.thera-bandacademy.com/exercises/showroutine.asp?erID=46&disease=12&t=9%3A09%3A07+PM
http://www.thera-bandacademy.com/exercises/showroutine.asp?erID=46&disease=12&t=9%3A09%3A07+PM
 http://strozpt.com/Stroz_PT/Balance_&_Vertigo_Rehabilitation.html
http://strozpt.com/Stroz_PT/Balance_&_Vertigo_Rehabilitation.html
Sit to stand
- Forward weight shift activities increase motor control in trunk and in LEs to allow for weight transition.
- Partial sit to stand with UEs supported on mat table
 http://www.lynden-hill-clinic.co.uk/html/healthcare/strokes_CVA.htm
http://www.lynden-hill-clinic.co.uk/html/healthcare/strokes_CVA.htm
Kneeling
- Half-kneeling: stabilization emphasis is on the posterior limb: allows for distal control of front leg and proximal control of back leg

Video Of Half-Kneeling Dynamic Activity
Modified Plantigrade
- Weight bearing on all extremities increases stability offered from trunk and facilitates knee extension

Standing
- Parallel bar progressions allow for B UE weight bearing in functional positions for transition to assistive device
- Anterior-posterior and anterior-lateral, posterior-lateral weight shifting with and without UE support for pre-gait sequencing
- Integrate weight-bearing patterns or restrictions as needed depending on the patient case
 http://www.lynden-hill-clinic.co.uk/html/healthcare/strokes_CVA.htm
http://www.lynden-hill-clinic.co.uk/html/healthcare/strokes_CVA.htm
Locomotion - Gait
- Parallel Bars: Sit to stand, stand, dynamic standing, ambulate, turn, return to sitting
- Indoor Overground: walking forward, backward, resisted walking, sideways and braided walking, step ups, walking with head turning, increasing walking speed/distance, decreasing use of assistive device
- Outdoor Overground: curbs, ramps/slopes, uneven terrain (grass, gravel, etc.), on/off escalators, crossing with traffic lights, open environments (shopping malls, school halls, etc., transit depots)
- Body weight support:
- canes, LBQC/SBQC, crutches, walkers, body-weight supported treadmill training, LiteGate
Recent evidence notes improvements in gait speed in seniors who engage in yoga exercises (Kelley, Aaron, Hynds, Machado, & Wolff, M, 2014).
Considerations for the Patient with Neurological Dysfunctions
- Mild to moderate motor impairments following stroke can have significant implications for locomotion
- 40% are limited to ambulating household distances
- approximately 70% experience a fall within the first 6 months following stroke
- patients post-stroke are ten times more likely to sustain a hip fracture
- participation in social activities is directely correlated to independence with community-level ambulation
Therapeutic exercises to improve or increase gait may include manual techniques and assistive devices to increase sensorimotor integration and proprioceptions. Examples of techniques include
- custom AFO or KFO for proprioceptive feedback and stability during weight bearing
- theraband straps to involved LE for increased proprioception and facilitated stepping
- visual cues (mirrors, colored tape on floor, colored signs in hallways) for visual feedback on midline orientation, accuracy, and to practice visual scanning while walking
- metronome or other audio cue (e.g., music) to increase cadence or ability to initiate stepping
- ankle and wrist cuff weights to decrease ataxia from cerebellar lesions
- partial weight-bearing supported gait activities on a treadmill
- hippotherapy (horse-assisted interventions)
Technology-enhanced advancements
Virtual reality, game-based immersion simulation, and exoskeleton technologies are developing and are progressively introduced into rehabilitation settings
Active Learning Exercise
Now it's time to work on your observation skills and apply your prior knowledge of neuromuscular examination elements, neuromuscular tests and measures, and treatment techniques:
I have created a TEDEd video that guides you through a clinical scenario, and includes self-reflection prompts and discussions. Post your responses directly in the TEDEd videw when prompted
References
Kelley, K. K., Aaron, D., Hynds, K., Machado, E., & Wolff, M. (2014). The Effects of a Therapeutic Yoga Program on Postural Control, Mobility, and Gait Speed in Community-Dwelling Older Adults. Journal Of Alternative & Complementary Medicine, 20(12), 949-954. doi:10.1089/acm.2014.0156
O'Sullivan SB, Schmitz TJ. Physical Rehabilitation. 5th Ed. Philadelphia, PA: F.A. Davis Company; 2007.
Stein J, Harvey RL, Macko RF, Winstein CJ, Zorowitz RD. Stroke Recovery & Rehabilitation. New York, NY: Demos Medical Publishing, LLC, 2009.

