FN
225:
Nutrition
Tamberly Powell, M.S., R.D.
Health Professions Division
Lane Community College
Eugene, Oregon
FORUM for Week 9:
The first link below is a summary of an article that looked at whether
different genotypes were more successful with losing weight with a
low-fat versus a low-carb diet. The second link is the published
peer-reviewed journal article of this research for those who are
interested in the scientific details.
As you read this (or even just watch the 4 minute video in the first
link), how does the information align with what you are learning in this
course? How is the information different? What can you take away from
this research and apply to your own eating?
What do you think of the 4 parts of "The Nondiet Approach" listed at the end of Lecture 9A
and how might you be able to apply this to a health care profession?
LECTURE 9A: Chapter
11- Achieving and Maintaining a Healthful Body Weight
First consider the major headings of this lecture:
There are many formulas you can use to calculate a
healthy body weight (and we will discuss some of these later), but I
love how the text describes a healthy body weight:
A weight that is appropriate for your age and
physical development
A weight you can achieve and sustain
without severely curtailing your food intake and constantly dieting
A weight that is compatible with normal blood
pressure, lipid levels, and glucose tolerance (in other words you
are metabolically fit)
A weight that is based on your genetic
background and family history of body shape and weight (after all
the apple does not fall too far from the tree)
A weight that promotes good eating habits and
allows you to participate in regular physical activity
A weight that is acceptable to you
Overall, a healthy size should not be dictated by a
formula, or the latest fad or societal expectations. Healthy sizes
come in all shapes and sizes, and you have to determine what a healthy
size is for you.
B. Body Mass Index (BMI)
BMI is a commonly
used equation to determine degree of obesity. It is a ratio of a
person's body weight to the square of his or her height. You can use the
following equation to calculate BMI:
BMI = [weight (lb)/height
(in2) ] x 703
BMI puts people into one of five weight categories
which is related to a certain health risk:
Underweight
(BMI < 18.5) which is associated with increased risk of health
problems.
Normal weight (BMI from 18.5-24.9) is
associated with the lowest health risk.
Overweight (BMI from 25-29.9) puts people
at a higher health risk.
Obese (BMI from 30-39.9) which increases
the risk of diabetes, heart disease and other chronic diseases
significantly.
Morbidly Obese (BMI of 40 or above)
putting someone at very high risk for disease.
The Body Mass Index
correlates significantly with body fatness, however it is
most accurate in determining the degree of obesity, and less useful in
determining nonobese people’s body fatness. Two drawbacks to BMI is
that it fails to indicate how much of the weight is fat and where the fat is located. The
location of fat is important because people who store fat more centrally
(apple shaped) have a higher risk for chronic disease compared to people
who store fat in the hips, thighs, and buttocks (pear shape).
Using just the BMI, at the time of this photo, Michael Jordan would have been considered obese,
since BMI does not distinguish between fat and lean body tissue.
C. Measuring Body Composition
DEXA scan.
Although this is the most accurate way to measure
body composition, it is very expensive and is usually just done in medical settings.
Underwater weighing.
Traditionally, underwater weighing has been considered the most accurate way to measure body composition. This is based on the principle that
fat
"floats".
A person is first weighed. They then exhale as much air as
possible and are immersed under water for 10 to 15 seconds for an
underwater weight measurement to be taken.
This procedure is repeated 7 to 10 times. Total test procedures may require 45 minutes to one hour.
This technique is not measuring body fat, but body density,
which translates mathematically into percent body fat. During
translation, however, significant error can creep into the picture.
Error can also happen with using weighing systems that lack precision,
and inexperience from the person being weighed. (Clark, 2014)
Fatfold test. Skinfold calipers are
a convenient and inexpensive way to measure body composition. Keep
in mind the accuracy of calipers will depend on the skill of the person
taking the measurements, the accuracy of the calipers, and the
appropriateness of the conversion equations. A suitable use is for one
person to do the measuring, then the SAME person do it after 3
months or so to see if there's been a change. Repeated measurements by
different technicians, using different calipers, and different
conversion equations will yield very different results (Clark, 2014).
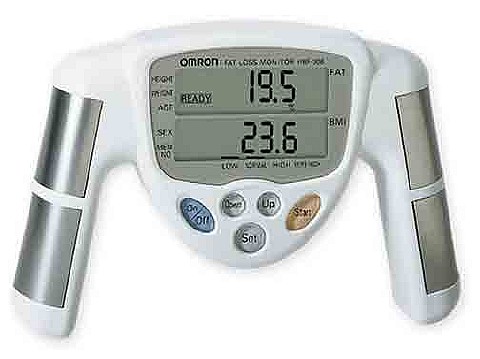
Bioelectrical impedance. Bioelectrical
impedance analysis measures body composition by sending an
imperceptible electrical current through the body. The amount of
water in the body affects the opposition to the flow of the current
(impedence). Because water is found only in fat-free tissue,
the current flow can be translated into percent body fat. (Clark,
2014) Limitations of this include body fluid levels must be normal
which can be impacted by exercise, alcohol, and menstrual cycles.
Above is a hand-held device for measuring body composition using bioelectrical impedence.
This is a scale you can stand on and measure body
composition using bioelectrical impedence. Students have told me
that there are much cheaper ones available, but I'm not sure of their
accuracy.
"Bod Pod".
This is a fairly new way of measuring body composition and the one pictured below is at the UO Treatment Center beside Autzen
Stadium.
While a person sits inside the enclosure, a rapidly vibrating diaphragm
in the wall of the test chamber produces small changes in air pressure
between it and an adjoining reference chamber.
The changes in air pressure can be used to determine the amount of air
the person displaces in the test chamber. In turn, that measurement
leads to an estimation of the person’s body volume, corrected for
the volume of air in the lungs at the time of the measurement.
Then, taking the person’s body mass (obtained by a scale) and
dividing it by the person’s body volume, the body density is
determined. With that, a person’s percent body fat can be
calculated.
Keep in mind that body composition can be hard to measure
accurately. Your best bet is to pick one method, and use that
method over time to compare numbers and see how they change. But don't
get too hung up on the actual number as the accuracy will be
questionable depending on the method chosen.
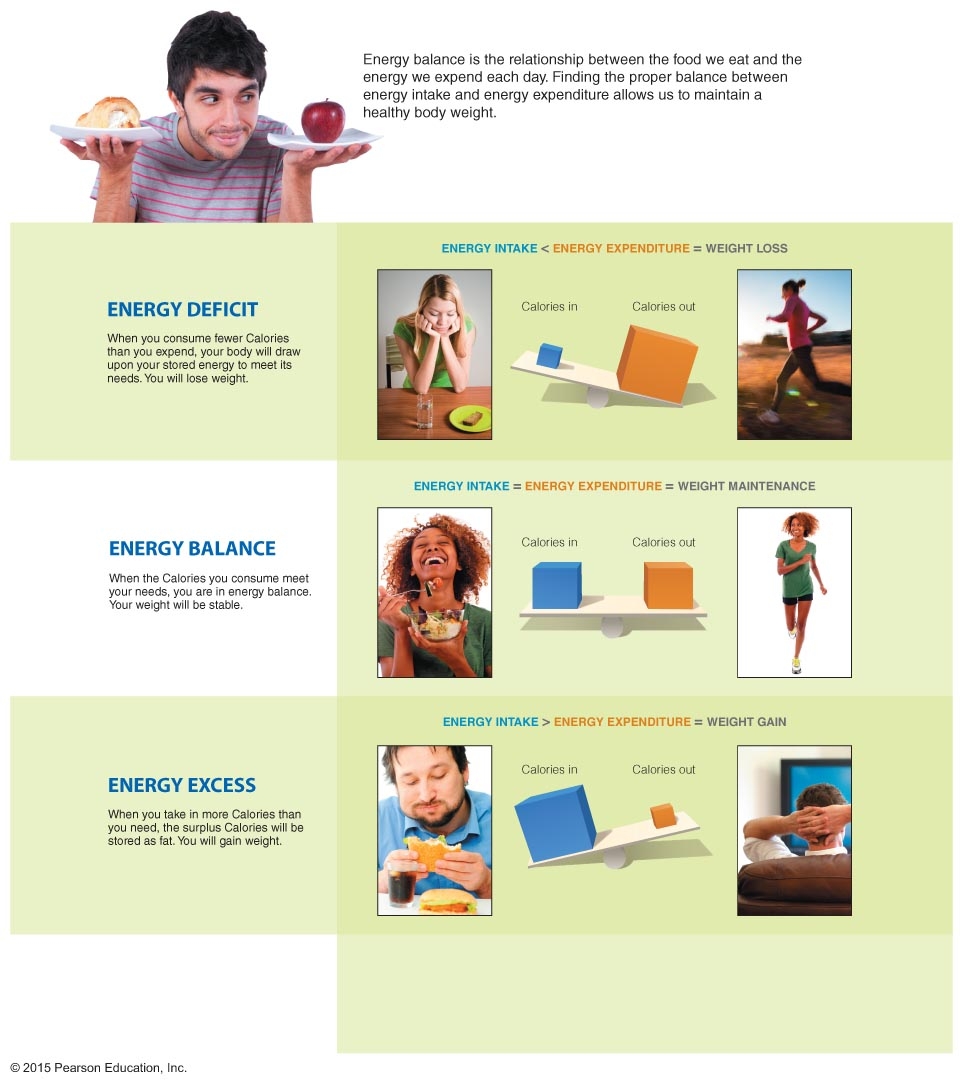
Our body weight can fluctuate based on our energy
intake (foods we eat) and our energy expenditure (energy we expend
during rest and physical activity). This relationship is defined by the
energy balance equation.
Energy Balance = energy in - energy out
Positive Energy Balance means energy in > energy out
(Weight Gain MAY result)
Negative Energy Balance means energy in < energy out
(Weight Loss MAY result)
Equilibrium means energy in = energy Out
The image below illustrates this.
If you consume 3,500 more Calories in
a week than your body needs, you COULD gain one pound, because a
pound of fat is equal to 3,500 Calories.
If you expend 3,500 more calories in a week than
you take in, you could lose a pound.
Notice I say COULD. Although the concept of energy balance
seems simple it is a dynamic process and is influenced by many factors.
In a study of identical
twins who were given an extra 1,000 Kcals a day for 100 days some
set of twins gained less than 10 pounds, while others gained up to 30
pounds. People gain and lose weight differently, we don't
necessarily follow formulas. Below we discuss the factors that impact
energy balance.
B. Components of Energy Expenditure
There are three parts to energy expenditure (basal
metabolic rate, the thermic effect of food, and physical activity)
1.
BMR (Basal Metabolic Rate)
This is the energy expended by the body for its involuntary activities
to sustain life. Examples include:
The Basal Metabolic Rate does NOT include digestive or physical activities.
The number one determinant of BMR is the amount of lean body tissue we
have. Lean body mass is more metabolically active than fat tissue.
Therefore a male's BMR is generally higher than a
female's because a male body generally has a higher percentage
of lean body mass than a female body. A female body is
made to have a higher percentage of body fat because of
reproductive needs. Of course there are exceptions. A
female can surpass a male if her physical conditioning is more
regular.
If a person is sedentary or moderately active, BMR is
the body's largest energy expenditure. A sedentary person might
need about 1800 calories in a day, with about 1200 of them being for
the BMR.
An accurate way to measure energy expenditure is to measure oxygen use, since oxygen is needed to complete the Krebs cycle.
Here energy expenditure is being measured for horse
racing on an equine simulator.
2.Physical activity is the other important way the body expends energy.
Physical activity can contribute anywhere from 15-35% of energy
expenditure.
Examples of physical activity would be unplanned activities like dashing to class or planned activities like lifting weights or swimming.
3.
Thermic Effect of Food (TEF)
This is the energy needed to digest, absorb,
transport, metabolize, and store the nutrients we need. About 5 to 10% of calories in a food are lost
because of TEF.
C. Genetic Factors
1. The FTO Gene-
There are more than 120 genes that are thought to be associated
with an increased risk of obesity. One gene that has got a lot of
attention is the FTO (fat mass and obesity-associated) gene. It is
estimated that 45% to 65% of people have at least one
copy. This gene seems to stimulate excessive food intake and reduce
satiety.
2. The Thrifty Gene Theory- This theory
suggests that people may have a gene (or genes) that causes them to
expend less energy than people with out this this gene (they are
energetically thrifty). Although this gene has not been identified
yet, this theory has been applied to populations who have experienced
severe feast and famine (Native Americans) who might have benefited from
a thrifty gene. But now consider people with this gene in our
current food environment and how it can work against them.
3. Set-Point Theory- This theory suggests that
our body fights to maintain our weight within a certain range or "set
point". So if we dramatically decrease our calorie intake (fasting or
very low calorie diet) our body responds with decreasing our basal
metabolic rate which would reduce energy output.
D. Diet Composition- A balanced diet that
follows the dietary guidelines for fat, carbohydrate and protein will
provide the most satiety. In other words it is a diet that will
fill us up with nutrient dense foods and keep us fuller longer.
1.
Foods high in sugar are especially tempting and research shows foods high
in rapidly absorbable carbohydrates (sugars and refined starches) may
promote eating more in general and create a reinforcing loop for
overconsumption of additional rapidly absorbable carbohydrates. (Lucan
and DiNicolantonio 2014)
2. Processed foods are major sources of the
nutrients we generally get too much of, including calories and sugar.
Processed foods contribute 75% of our addedsugar. (Katz,
2014)
E. Metabolic Factors
1. Having a low metabolic rate.
2. Having a low level of spontaneous physical
activity. These are activities like fidgeting or pacing.
3. Having a low fat oxidation which means fat will be
stored and more carbohydrate will be burned for energy.
F. Physiological Factors
1. Hunger and Appetite- There could be genetic variations in perceptions of hunger and appetite.
Hunger is the
physicalneed to eat. Physical
symptoms include our stomach growling and feeling light headed.
Appetite is the psychological desire to eat creating satiety (feeling
full).
Some people may not have the ability feel full (an
insufficient satiety mechanism) which causes them to over eat.
2. Energy-Regulating Hormones- Genes direct the making of
ghrelin, a
peptide hormone produced by the stomach. Ghrelin stimulatesappetite and increases food intake. Levels of this hormone
increase before eating, and then fall within 1 hour after eating.
Therefore, it is thought that ghrelin plays a role in both hunger and
appetite. Ghrelin levels appear to increase after weight loss,
which may contribute to the difficulty of maintaining weight loss.
Genes in fat cells direct the making of leptin, also a
peptide hormone, but one that is produced by adipose (fat) cells. It plays
a role in body weight regulation by acting on the hypothalamus to
suppress appetite and burn fat stored in adipose tissue. Obese people
lose their sensitivity to leptin.
Perhaps the brain cells of obese people ignore leptin, just as
some diabetics' cells (Type 2 diabetics) ignore insulin.
Eve Van Cauter, an endocrinologist at the University of Chicago who is shown above, calls ghrelin and leptin the “yin and yang" of eating regulation.
In experiments by Van Cauter and
others, sleep-deprived adults produced more ghrelin, a hormone that
promotes hunger, and less leptin, a hormone that signals fullness.
G. External Factors (which include Cultural, Economic,
and Social Factors)
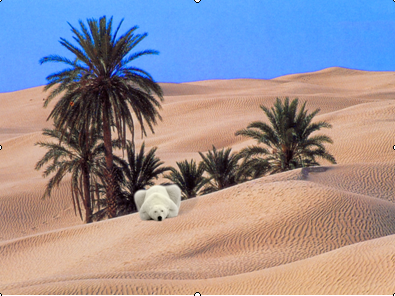
I saw the below image at a conference I went to on
obesity, where the speaker was comparing our current situation (a
body that is set up to deal with scarcity, not abundance, in an
environment where we have every reason to over eat, and not move) to a
polar bear in the Sahara dessert. A polar bear is designed to
withstand frigid temperatures, not heat. We physiologically are
wired for hunter and gather lifestyles where we have to work really hard
for precious Calories in return. When we are put into our current
"toxic" food environment our bodies go haywire, and as a result are
developing chronic diseases like heart disease and diabetes at alarming
rates.
1. Lack of Exercise
There are all sorts of
reasons why we're getting less exercise these days. One of them
is the lack of PE classes in schools. They've been a casualty of
decreased school funding and
the increasing pressure for schools to focus on academics so students score well on state-wide academic tests.
We also have more sedentary jobs and rely on more
labor-saving devices today.
2. TV. Nutritional problems
with excess TV watching:
Although some people work out when watching TV, many of us are not moving much, so it takes away from the hours
of moving in the day.
And TV can have what I call the "zombie effect". Two of the
children in the photo above have parents who were LCC nutrition faculty
at the time and
watching TV turned them into "zombies".
Research has shown that while watching TV, BMR falls even lower than just sitting around when you're not watching TV.
People often mindlessly snack when they're watching
TV. Since they're not really paying attention to what they eat,
they may eat more than they need to be satisfied.
Many TV ads are for highly processed and high calorie foods and the ads make you want the food.
Many of the actors and actresses on TV have
unrealistic body shapes which might encourage eating disorders.
3. Marketing is a big external cue that encourages us to eat. Watch the following clip on food marketing.
4.
Weight Cycling is the on again-off again dieting that some people experience.
We get all sorts of cues in our culture that dieting is a good thing.
But weight loss diets seldom are successful in achieving
long-term weight loss. Instead, what can happen after successful
weight loss is that the person begins overeating, gaining more weight
than what they weighed before the diet. This will be discussed more in lecture
9B.
A. During the 1st day of not eating your brain and nerves get energy from glycogen in your
liver.
Your brain isn't set up to get energy from the glycogen in
muscles. Glycogen in muscles can only
be used for that muscle.
The body stores about a pound of glycogen. About 3-4 pounds of water is wrapped around that pound of glycogen. On a
fast or a low carbohydrate diet, you lose that pound of glycogen because it is being broken down to provide glucose for the brain.
On a
fast or a low carbohydrate diet, when you lose that pound of glycogen, you also lose the 3-4 pounds of water
that is wrapped around it. So you would lose 4-5 pounds during the first day or 2 of a fast.
This is why low carbohydrate diets are so tempting. Low carbohydrate diets do work to provide rapid and dramatic weight loss. The problem is that most of that weight is water and it's a temporary weight loss.
As soon as you eat foods with carbohydrate (which your body will
drive you to do since the brain needs glucose), the glycogen will
come back, as will the water that wraps around that glycogen.
Your body is not happy being deprived of carbohydrate because
it wants glucose for the brain and fat can NOT be turned into a
significant amount of glucose. If you are not eating enough
whole foods with starch and sugar, your body has to change some of its
body proteins into glucose. Your body doesn't have a reserve of
proteins. Those proteins would come from the necessary protein of
muscles, enzymes, antibodies, etc.
B. During the 2nd day,
protein in muscles
& other places gets rearranged into glucose.
This decreases the amount of lean tissue in the body.
If this kept happening, the body could only survive about ten days.
Body fat cannot be rearranged into glucose in any significant amount.
Regarding what is meant by the statement "carbohydrates spare
protein", you should be able to answer this now, if not please post your
question(s) in the FORUM.
C. After 2 weeks of fasting, the brain has
learned to use ketones for about 1/2 of its energy needs, but
the other half still comes from protein in muscles &
other places (unless you're eating lots of protein, but this wouldn't be
happening with fasting).
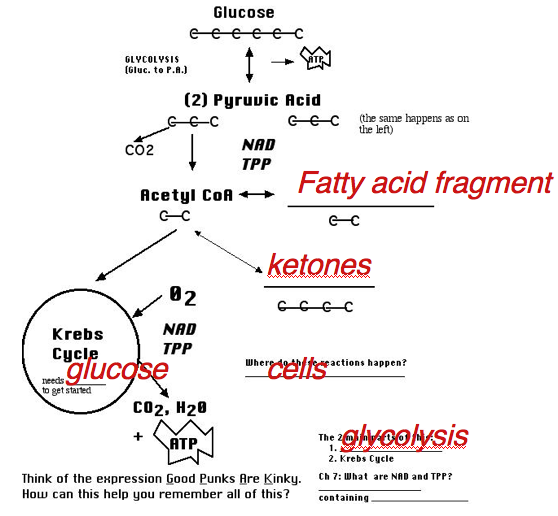
Ketones come from fatty acids fragments. They are made when there is a lack of glucose in cells
because the Krebs cycle needs glucose to get started. Without
glucose the fatty acid
fragments can't go through the Krebs cycle as quickly as they are being broken
down so they instead get made into ketones.
Three examples of situations that might lead to ketosis are:
starvation from poverty or anorexia or
uncontrolled diabetes where there is not enough insulin or the
cells don't respond to the insulin to help glucose get into cells.
Someone eating a very low carbohydrate diet (< 50
g/day).
After about 2
weeks of fasting or following a very low carbohydrate diet, the body's rate of lean tissue loss goes down because
the brain relies more on ketones for about 1/2 of its energy
needs.
The brain is able to utilize ketones as an energy source by making
enzymes to help the brain break down ketones.
But
the other half of the brain's energy still comes from protein in
muscles &
other places (unless you're eating lots of protein). Someone
fasting for weeks at a time can still die from loss of essential
protein tissue, even if they still have fat reserves.
IVPossible Causes
[maybe "contributors" would be a better word]
of Eating Disorders (especially anorexia)
As we seek to understand another's problems, it's tempting to blame
someone (like the person or the parents) and comfort ourselves
that the same thing won't happen to us if we just don't do what the
other person is doing wrong. But in addition to not being
helpful, that blame can make matters worse instead of better. It
is more likely that a supportive understanding can more quickly lead to
the help that is usually necessary for recovery.
A friend saw a bumper sticker once that said something like
“Children don't choose anorexia and parents don't cause
it.” What other people do can contribute to eating
disorders, but other people are not the cause. A person with several of
the following contributing factors doesn't mean they have to accept the
inevitable and adopt a “victim” mentality. But if it
does happen, quickly getting help can enable them to manage the
disorder so it can move to the background of their life.
These are my ideas about contributing factors.
Genetics.
Eating disorders run in families and it's easy to assume the
family environment led to the problem. Recent studies of twins,
presumably raised in the same environment, are finding a clear genetic
link. “In a large study comparing the number of identical twins
who had anorexia with the significantly smaller number of fraternal
twins who had it, scientists concluded that more than 50 percent of the
risk for developing the disorder could be attributed to an individual's
genetic makeup. A few small studies have even isolated a specific area
on the human genome where some of the mutations that may influence
anorexia exist, and now a five-year, $10 million NIMH study is underway
to further pinpoint the locations of those genes.” (Tyre,
Newsweek)
Twin studies have also looked at bulimia. “Women with bulimic or
anorexic female relatives are four to five times more likely to develop
the disorder, and twin studies reveal that the genetic risk factor may
be as high as 58 percent.” (Psychology Today)
Perhaps genes help create a brain chemistry that can
lead people to use starvation (or over-eating) as a way to control
anxiety. Serotonin is a chemical messenger in the brain made from
the essential amino acid tryptophan and it affects emotions, behavior,
and thought. Normal levels of serotonin are believed to be
associated with feelings of well-being. Both low and high levels
of serotonin may be associated with certain mental health
disorders. Both starvation and over-eating could be attempts to
return brain serotonin levels to normal. It has been suggested
that the brain of a person with anorexia may have increased serotonin
activity.
Control Issues. Most of us have a
desire to control what's happening in our lives, and in varying
ways. When we feel ourselves losing that control, some can
temporarily “go with the flow” until they can find
satisfying ways to re-gain it. Others may lash out with violent
behavior or seek escape with drugs or alcohol. Still others may
decide to use not eating or over-eating to feel a measure of
control. All of these ways of seeking control can have a genetic
basis, as evidenced by the incidence of alcoholism in families.
Culture. Our culture places
tremendous value on narrow aspects of image such as thinness. Rather
than pursuing their unique interests and goals, many who don't fit this
image become preoccupied and depressed if they don't naturally fit this
image. When they lose weight, some may tell them how good they
look. This gives the message that they didn't look good before
and they can feel they probably don't look good yet. So they keep
dieting and for some reason we don't understand, the eyes of a person
with anorexia see a fat person in the mirror, even when they're
dangerously underweight.
Stressful/Traumatic Events.
Examples I've seen include a teenager whose boyfriend teased her
because of her “thunder thighs” and broke up with her,
parents who insisted on dieting because their child was being taunted,
a parent's serious illness, the stress of college applications, a messy
divorce at age 40 and a high-school exchange living situation in Mexico
where the family was domineering and demanding. It's impossible to
avoid stressful and traumatic events, but empathy regarding the impact
of life experiences can be very helpful.
V
Do's for Family Members & Friends of People with Eating Disorders
(A list is in your lecture notes.)
So what should you do if someone you care about shows signs of an
eating disorder? Treatment seems simple- either eat if the
problem is under-eating or don't eat if the problem is
over-eating. But treating a person with an eating disorder as if
the treatment is simple can have an opposite-of-the-desired effect and
instead make the problem worse instead of better. One term, a
student told me “I developed an eating disorder a couple of years
ago at almost 40 years old during my divorce and the people around me
chose to try to discipline it out of me.” She told me that
attitude did not help her as she struggled to recover.
The Nondiet Approach (This list, which is in your
lecture outline, is from the book below.)
Total health enhancement and well-being, rather than weight loss or achieving a specific "ideal weight."
Self-acceptance and respect for the diversity of
healthy, beautiful bodies, rather than the pursuit of an
idealized weight at any cost.
The pleasure of eating well, based on internal cues of hunger and satiety, rather than on external food plans or diets.
The joy of movement, encouraging all physical activities rather than prescribing a specific routine of regimented exercise.
Comparison of Traditional Weight Loss Paradigm and Health at Every
Size (HAES)
Traditional
HAES
Everyone needs to be thin for good health
Thin is not intrinsically healthy and
beautiful nor is fat unhealthy and unappealing
People are overweight b/c they have no
willpower, they eat too much, and move too little
People naturally have different body shapes
and sizes and different preferences for physical activity
Everyone can be thin, happy, and healthy by
dieting
Dieting usually leads to weight gain,
decreased self esteem, and increased risk for eating
problems. Health and happiness are not dependent on weight.
How does your approach or thoughts about weight loss
compare to the above? Do you take more of a traditional approach
or HAES approach? Which approach do you think would be more
positive in a health care setting?