Review of Spinal Alignment
Normal spinal alignment has been introduced in PTA 101 and reinforced in PTA 133L and PTA 104/104L
- Spine should be vertically straight
- Center of occiput should be aligned with center of sacrum
- Results in normal lordosis (cervical and lumbar curves) and kyphosis (thoracic and sacral curves)
- Postural abnormalities are identified primarily through observation; decreases or increases in spinal curves at rest are consistent abnormal postural findings
Scoliosis
Scoliosis is any lateral curvature of the cervical, thoracic, or lumbar spine; rotoscoliosis is an updated term that is more specific to the abnormal combined lateral curve with progressive rotation at individual spinal segments
Primary Onset of Scoliosis
- classified as idiopathic: infantile (0-3yr), juvenile (3-9 yr), adolescent (puberty to adult), or adult
- congenital - some correlation with family history
- idiopathic (cause unknown) is the most prevalent form
- 75%-85% of all recognized types of scoliosis
- idiopathic adolescent scoliosis comprises about 80% of scoliosis cases
- R thoracic is the most common
- neuromuscular causes, such as imbalances in tone, spasticity, or loss of muscle function (paresis and/or paralysis)
- degenerative disease
Associated Symptoms
- pain
- decreased cardiopulmonary function (usually with thoracic curves greater than 65 degrees)
- decreased digestive function
- neurological symptoms associated with spinal stenosis.
Sample scoliosis progression (Approximately 2 minutes)
![]()
Secondary Onset of Scoliosis
- osteoporosis
- trauma (e.g.,, fracture, leg length discrepancy)
Prognosis
- Prognosis is influenced by:
- age of onset - Younger age-onset is has a poorer prognosis
- type of curve - Double curves have a poorer prognosis than single curves
- degree of curve - the higher the degree, the greater expectations of comorbidities and functional changes. Severity is classified by degree of curve
- curve <= 25 degrees - monitor for changes
- curve 25 to <=40 degrees - use of orthotic; physical therapy is recommended
- curve > 40 degrees may result in surgical stabilization to prevent further progression
- gender - biological females have a 10 times greater risk for progression
Classifying Scoliosis
Recognized as either structural or nonstructural
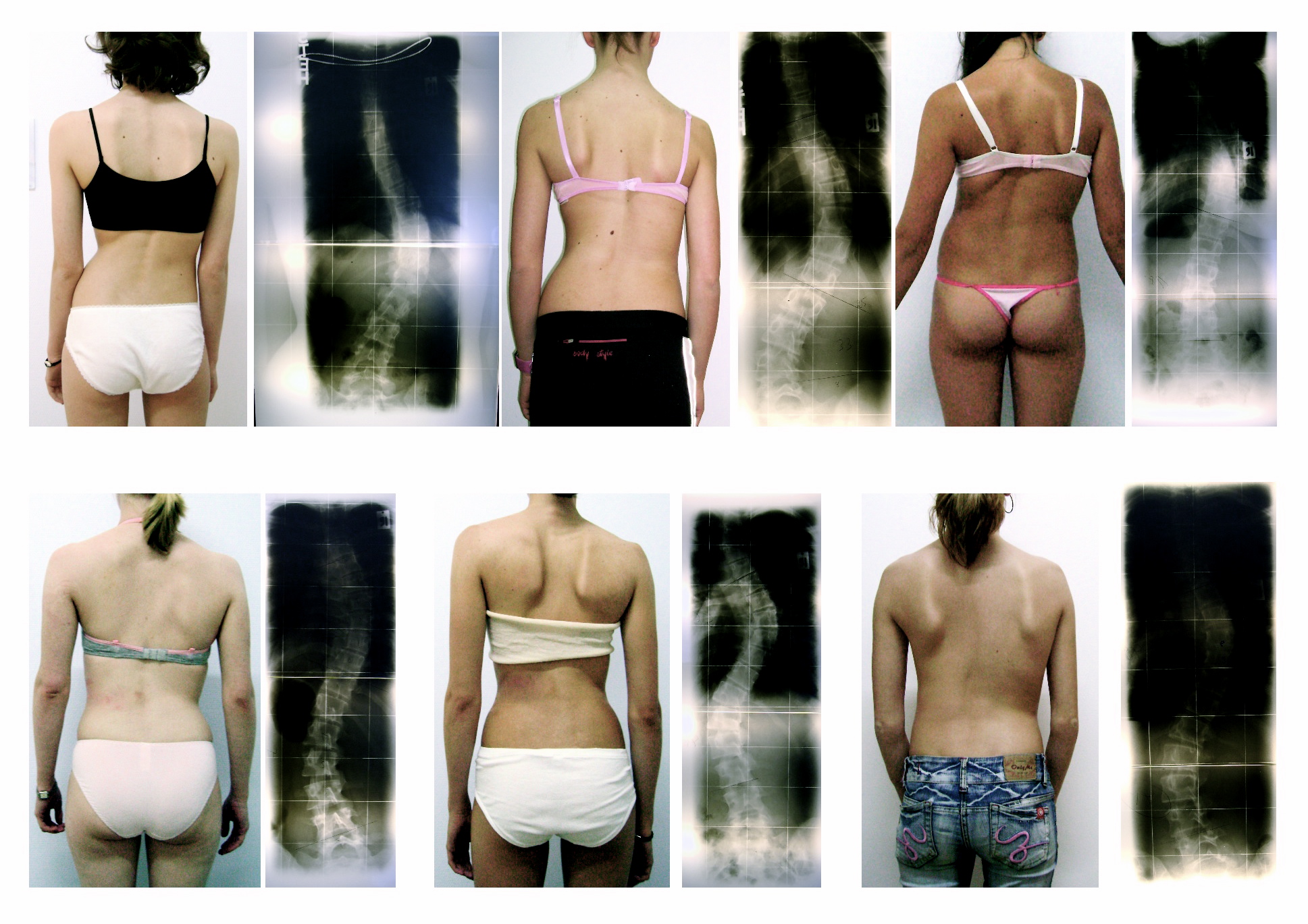
- structural: rotation of the spine is fixed, irreversible; lateral curves do not change with patient position or voluntary movement. The images below are examples of structural scoliosis
- non-structural: rotation of the spine is reversible; lateral curves are reduced with positional changes
Document observation findings to describe the scoliosis. Common documentation elements include:
- Side of the convexity: e.g. Right thoracic scoliosis
- Spine involvement: e.g., Right thoracic scoliosis
- Presence +Adams Forward Bend Test - rib hump during forward flexion indicates structural scoliosis named by side of convexity - direction of rotation
![]()
- Number of rotation curves - single vs. double