Basic Concepts of Spinal Management with Movement
Note: All images in this section are attributed to: Olson S, VHI Exercise Images , Tacoma, Washington:Visual Health Information, 1999
All patients should be engaged in motor learning and training regardless of their functional level. Specific training elements include:
- Kinesthetic Training: patient education on safe spinal motions with integration and application to activities of daily living
- Functional Training: applying principles of body mechanics during everyday activities, including prevention
- Stabilization Training: accessing and contracting muscles which provide spinal stability during gross motion
Elements of Kinesthetic Training
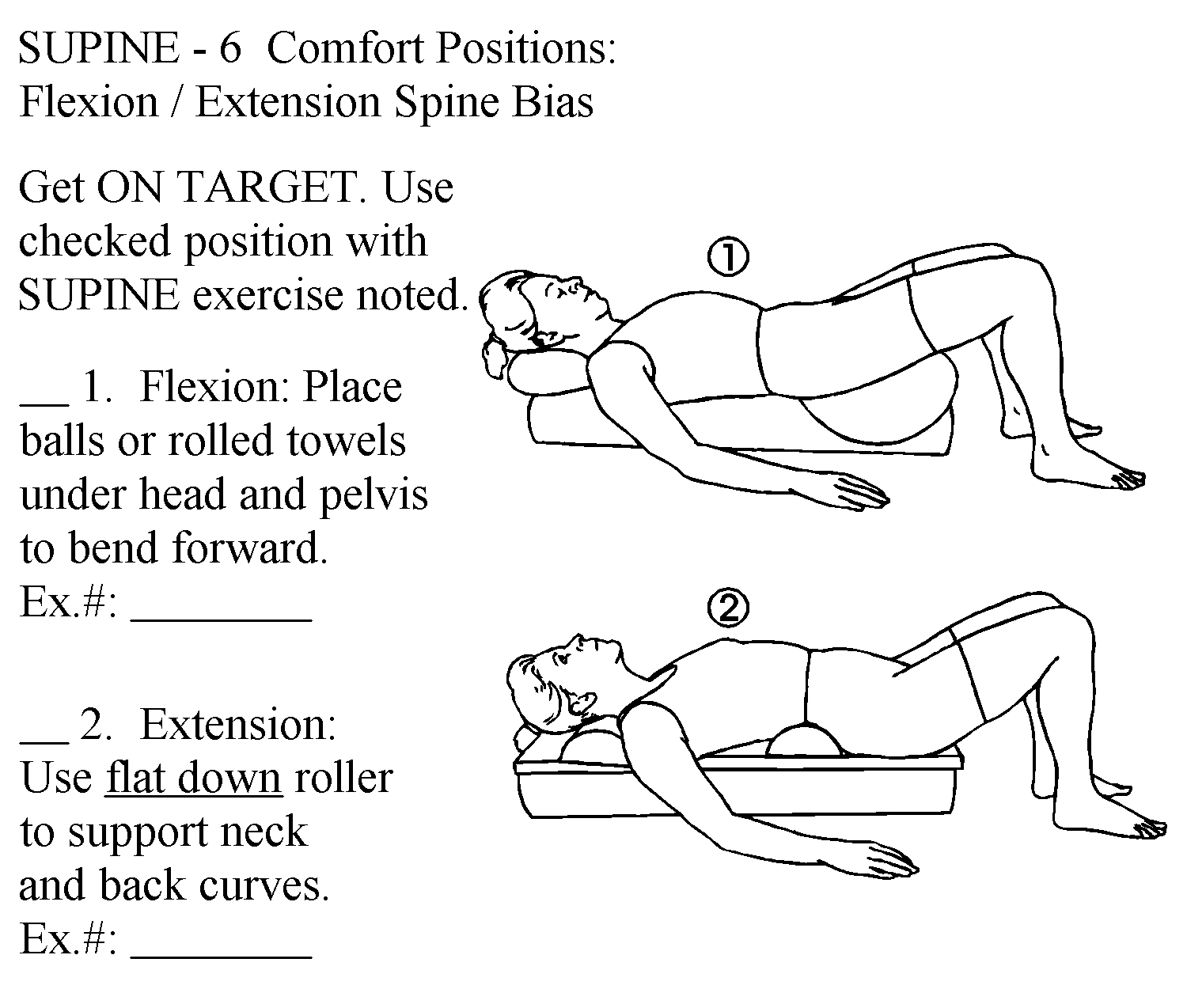
Position of bias = position of symptom relief; also known as the "resting position". This image shows how to teach a patient to use the position of ease for comfort.
Neutral spine = spine segments maintain neutral motion in all planes while in a position or performing a movement.
Emphasis is on bringing the patient's attention to what reduces symptoms and what aggravates symptoms and then educating and instructing them on methods to find and use positions of relief or methods to assume and maintain a neutral spine as a therapeutic activity.
The goal: increase awareness of muscle imbalances, or habits that lead to spine imbalance, and understanding of how these length-tension relationships affect symptoms.
Kinesthetic Training Examples
Recall from PTA 101L when you practiced moving into anterior and posterior pelvic tilt, then found your "neutral". You used kinesthetic awareness and instructions and feedback from faculty to inform your understanding of how to find that "neutral spine". Here are some other examples of kinesthetic training for function:
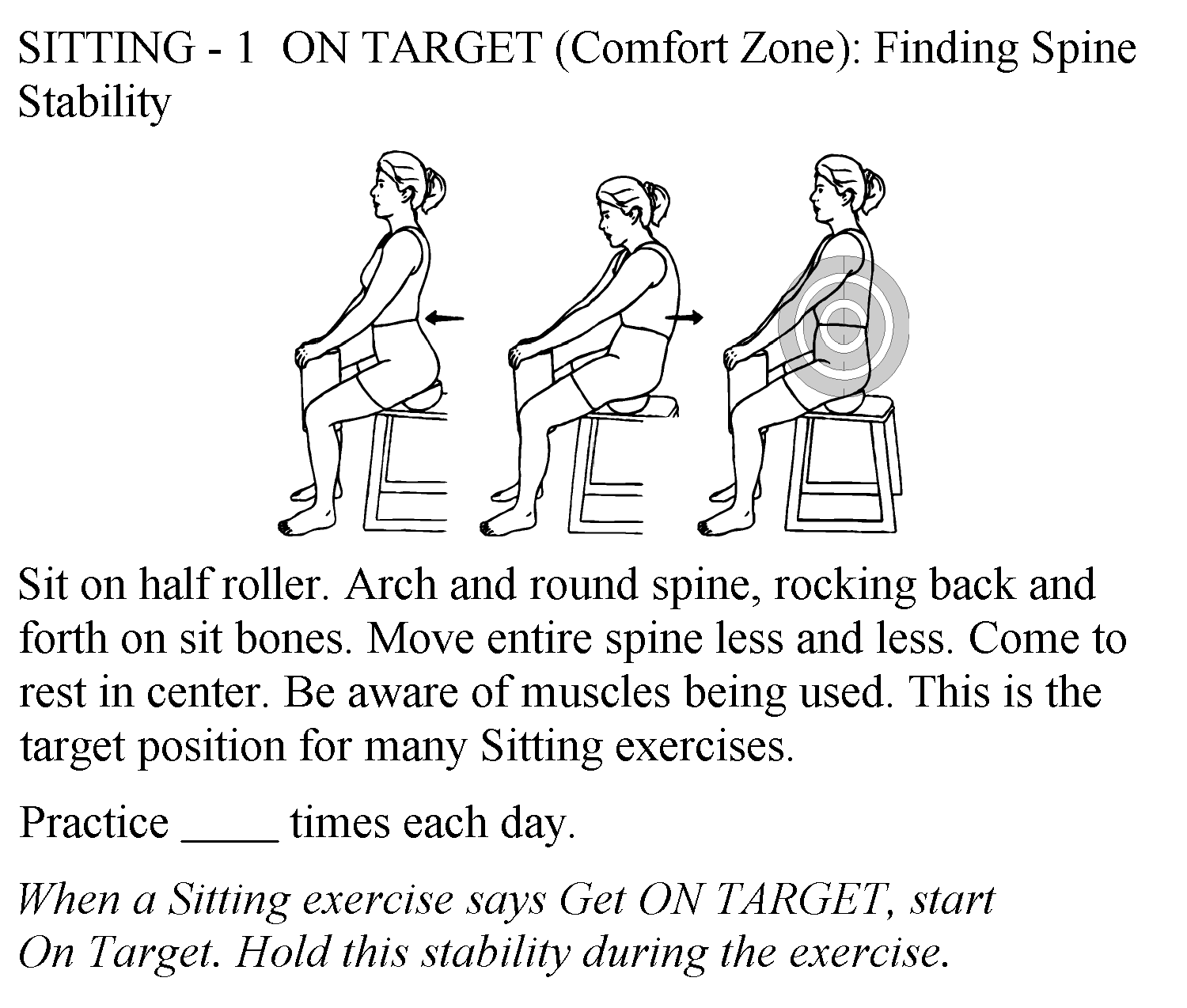
- facilitating movements between "slouched" and neutral posture in sitting and standing
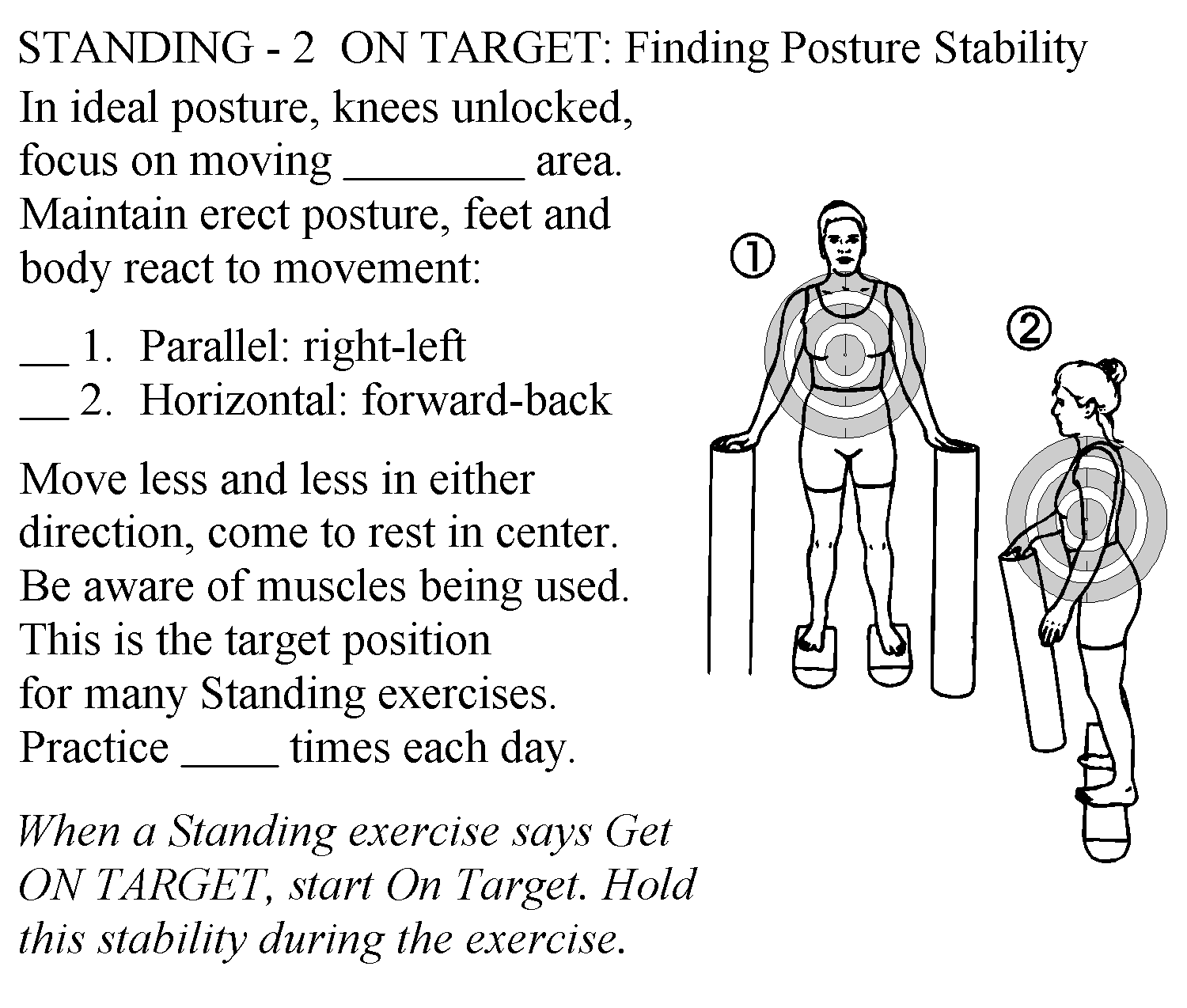
- using fixed objects, like doors and walls as a kinesthetic reference
- using your hand or the patients hand to provide feedback when unwanted movement occurs during a stabilization activity'
- noting signs of tight structures during movement by perceiving compensations
- allowing the patient to feel what takes place at the lumbar spine during prone knee flexion (tight hip flexors);
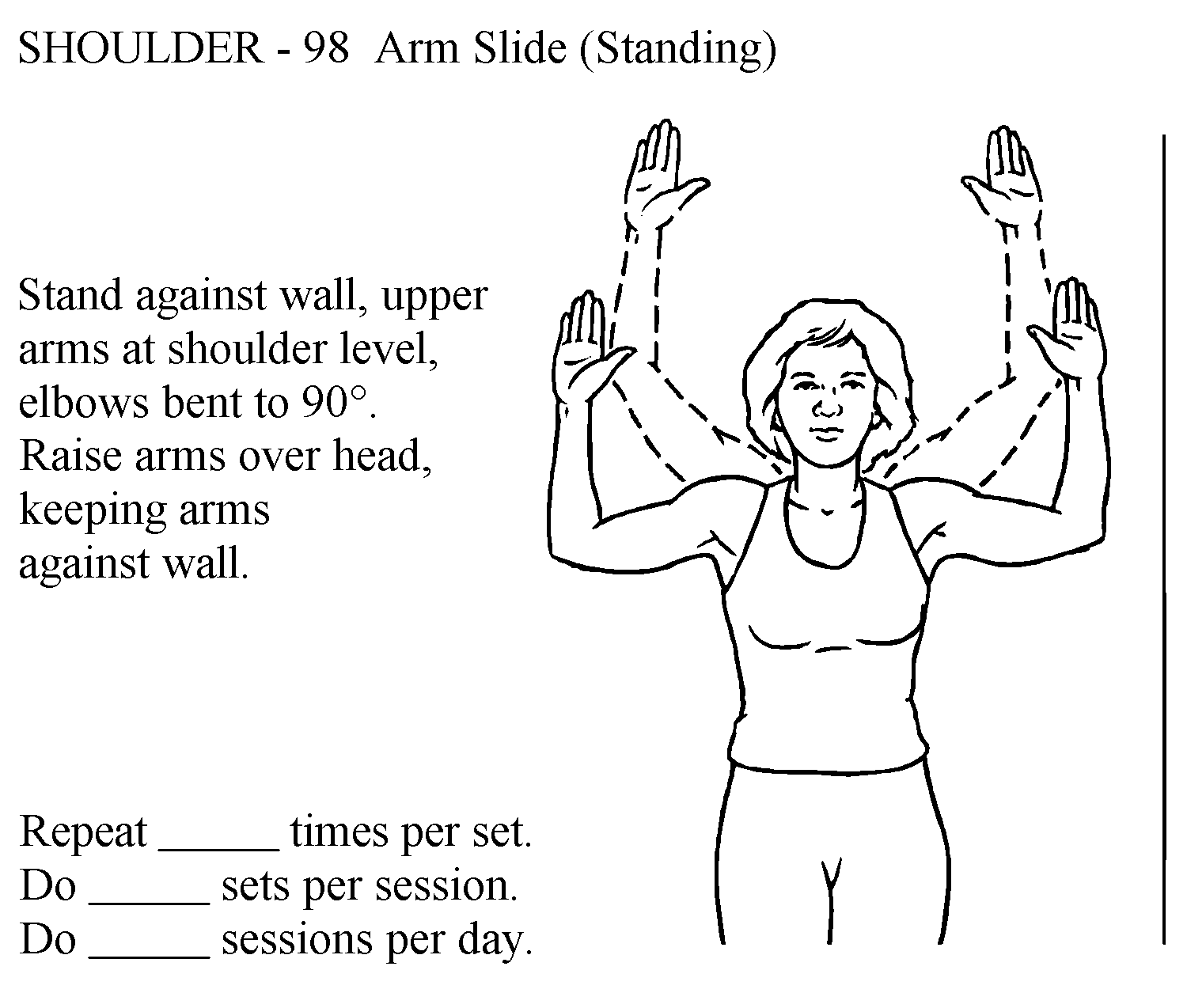
- allowing the patient to feel how head position will shift forward when reaching overhead (tight chest and restricted scapula);
- allowing the patient to see a Trendelenberg sign with single limb stance activities.
Examples of Kinesthetic Training in Cervical Spine
- Facilitated passive ROM with verbal cues with transition to active-assisted and active range of motion.
- common affected muscles include SCM, scalenes, upper trapezius, pectorals, levator scapula, suboccipitals
- Patient is positioned according to symptom tolerance (WB vs. non-WB)
- Supine positioning when first learning these techniques is recommended.
- Walls and doorways can be used for transition to PWB
Examples of Kinesthetic Training in Lumbar spine
Priniciples of kinesthetic training are used when teaching a patient how to use passive positioning for symptom reduction and progression to submaximal exercises and mid-range motions. For example:
- Hook-lying is non-weight bearing. It is ideal for initiating kinesthetic training in pelvic tilt motions due to slight flexion in lumbar spine. Hooklying promotes posterior pelvic tilt and lumbar flexion. Hooklying is often a position of ease and can be used to to teach submaximal abdominal and low back exercise.
- Prone is non-weight bearing. Patients may lie flat or use a pillow under the pelvis to accomodate as needed. Prone can be used to train a neutral spine while activating low back, hip (extensor, rotators) and scapula muscles.
- Sitting positions can be used to place a patient in a position of ease for the lumbar spine. For example, sitting with feet propped on footstool promotes lumbar flexion; with feet flat and lumbar roll promotes extension; use of arm rests in sitting promotes decreased WB in lumbar spine
- Standing positions such as placing one foot on a stool/block promotes posterior pelvic tilt. More advanced techniques can include the use of dynamic surfaces, like foam rollers
Kinesthetic Training with Limb Motion
The goal: perceive no significant compensatory movement at the spine when performing progresive limb loading activities. Demonstrate neuromuscular control by activating primarily stabilizers (spine) and producing appropriate direction and force of primary movers.
Teach client how controlled and correctly sequenced limb motion influences control of spine symptoms during functional activities: rolling, sit to stand, bending, etc.,
Again - recall from your PTA 101L experience: how did you teach a patient to move from supine to sidelying to sit? You applied principles of limb loading to reduce forces needed to sit up, and part of this included awareness of sequenced movements and minimizing forces on the spine.
In this image, the patient is trying to control the position of the head and cervical spine while the chest opens and shoulders abduct. Any compensatory motion of the head and neck, like flexing away from the door or being unable to maintain arms against the wall, would be felt by the patient and practiced again to prevent compensation. These observations may also guide decision-making for stretching interventions.
Postural and Functional Training Elements
When there are imbalances in postural, passive and active exercises restore length-tension relationships. These exercises and movements are used to mobilize joints and soft tissues. The key element is that these are performed correctly and at low frequency intervals throughout the day. Traction forces are stretching forces which may be used to decompress inflamed nerve root structures, thus decreasing pain.
The goal: Minimize or eliminate restrictions that prevent assuming and maintaining a neutral spine during sustained positions and activities
Self-mobilization examples for areas of hypomobility:
- extending over a foam roller or towel
- extending over a chair
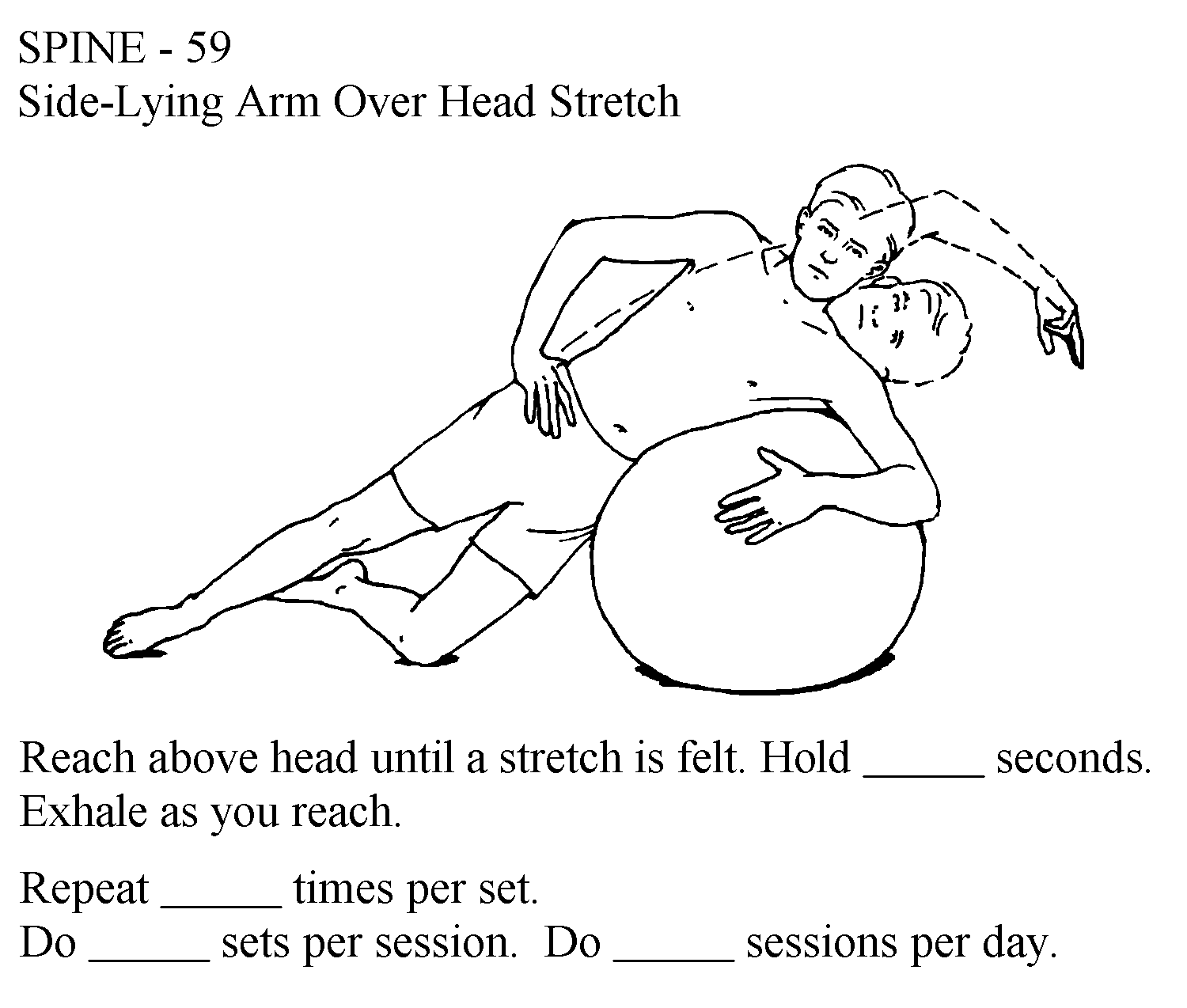
- sidebending over a therapy ball
- rotating over a fixed pelvis
- rotating over a fixed upper trunk
- quadruped rock (rocking back into heels) can help a patient identify posterior soft tissue restrictions or poor abdominal control
Functional training should be patient-specific as determined by the physical therapy plan of care. Patients should begin to practice basic functional training without the use of a load, then progressively work towards performing activities typical for their home and work environment.
In this example, a patient with a history of cervical pain would practice placing and removing moderately light objects on low surfaces while minimizing stress and strain to the neck using sliding shelves:
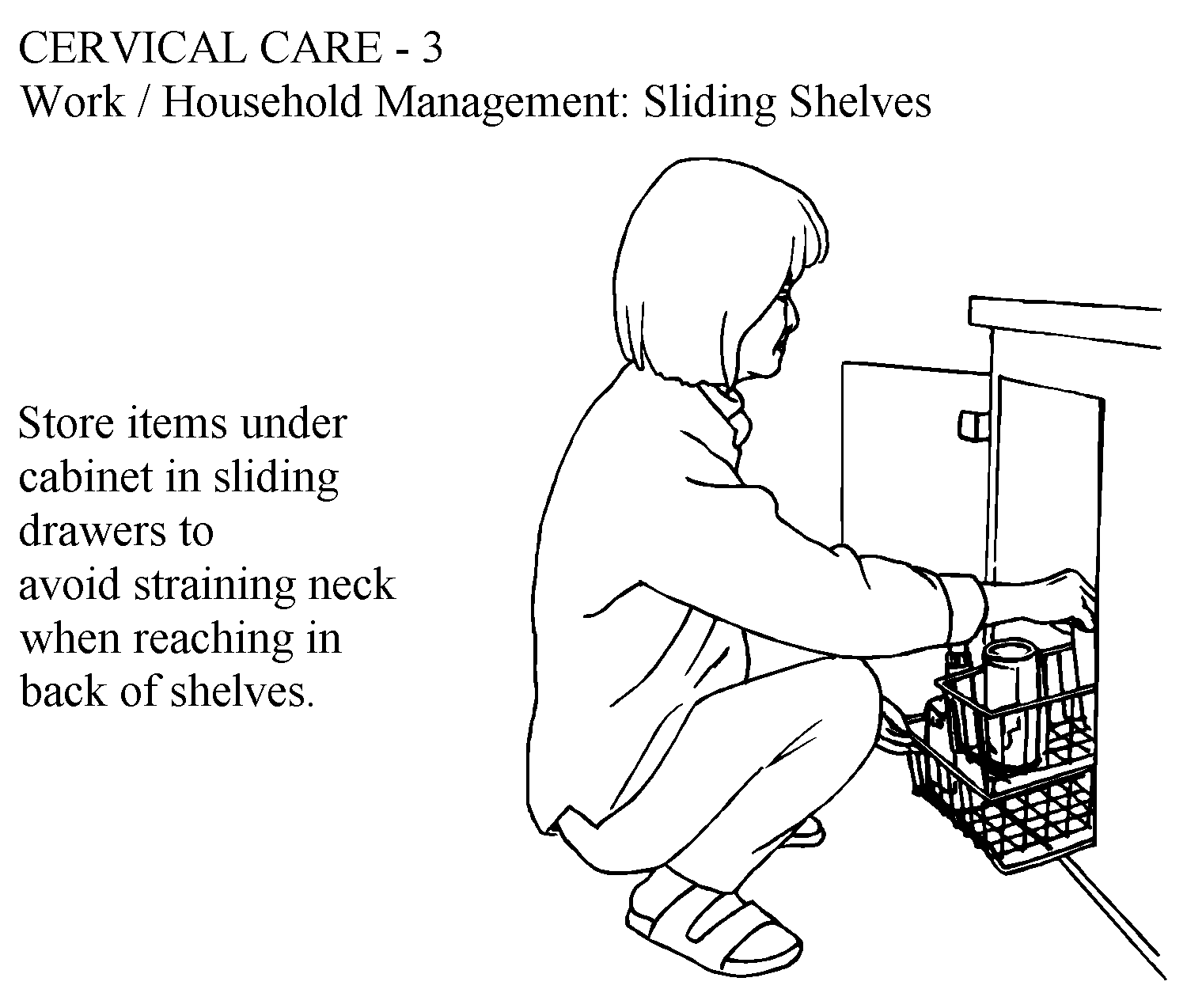
Work / Household Management: Sliding Shelves
Elements of Stabilization Training
The Dutton text provides excellent examples of these progressions for the cervical and lumbar spine
- Basic
- posterior pelvic tilt; cervical retraction
- drawing-in maneuver
- isometric multifidus contraction
- Intermediate - Spinal stabilization with limb loading - Notice the activities keep the body in double limb support, then progress to single limb support to increase control of flexion, extension, and rotation; although included as lumbar stabilization, consider the role of WB in UEs and limb movement on cervical and thoracic stability
- Hooklying heel slide
- Hooklying knee lift
- Hooklying bent knee fall out
- Sidelying clam shell
- Prone limb lifts
- single limb (arm/leg)
- double limb (arm leg)
- Quadruped limb lift
- single limb (arm/leg)
- opposite arm/leg lift
- Advanced - Focus is on increasing dynamic control with progressive increased resistance and decreased BOS to increase strength and endurance for return to function
- Side planks
- Side planks with limb loading (lifting arm or leg away from midline)
- Bridging (with double and single limb support, static and dynamic surfaces ( Bosu/Therapy ball, foam roll)
- Abdominal strengthening with limb loading
Shirley Sahrmann has adapted a sequence of exercises for spinal stabilization using limb-loading principles.
![]()
Video approximately 5 minutes
We suggest that you practice on your own or instruct a willing participant in each of the exercises. Many patients will need continuous feedback in the initial stages of learning and your own experience with practice can help you appreciate concepts of feedback and motor control
Self Checks


