


Thyroid Function and Condition
https://upload.wikimedia.org/wikipedia/commons/e/ed/ThyroidImage.jpg
Thyroid Hormone Physiology
The thyroid gland synthesizes and releases thyroid hormones which have diverse physiologic effects including cardiac, pulmonary, hematopoietic, gastrointestinal, skeletal, neuromuscular and endocrine effects (growth, reproduction, energy metabolism). T4, and to a much lesser extent T3, is released from the thyroid. Thyroid hormone synthesis is mediated by an enzyme called thyroperoxidase (TPO) and this enzyme is the target in Hashimoto's (autoimmune thyroiditis).
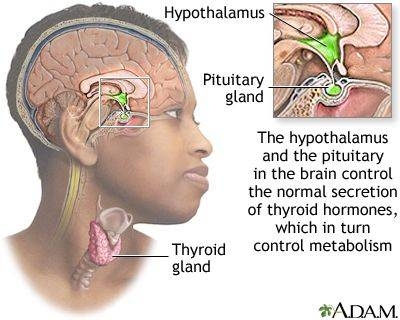
T3 is considered the active form of thyroid hormone. Thyroid function is regulated by the hypothalamic-pituitary-thyroid axis, shown in Figure 1. Synthesis and release of T4 and T3 are positively regulated by Thyroid Stimulating Hormone which, in turn, is positively regulated by TRH. Note the negative feedback by thyroid hormone on TSH secretion by the pituitary (as well as on TRH secretion by the hypothalamus).
| Figure 1. Hypothalamic-pituitary-thyroid feedback system for control of thyroid hormone secretion |
 |
Evaluation of Thyroid Function and Structure
Thyroid hormones are transported in serum bound to carrier proteins. The 0.04% of T4 and 0.4% of T3 that is free is the biologically active form.
Thyroid Binding Globulin (TBG) is the major thyroid hormone binding proteins. Alterations in thyroid binding proteins (especially TBG) will markedly change the total T4 and total T3 levels. Factors that influence thyroid hormone binding and therefore will alter total thyroid hormone levels include:
- Increased TBG (will increase total thyroid hormone levels)
- Congenital (rare)
- Estrogen (oral contraceptives, pregnancy, estrogen replacement therapy, feminizing tumors)
- Hypothyroidism (increase in available binding sites on TBG
- Acute hepatitis (release of TBG from liver)
- Intermittent porphyria
- Drugs (heroin, methadone, 5-FU)
- Decreased TBG (will decrease total thyroid hormone levels)
- Congenital (rare)
- Androgens (testosterone, DHEA-S, anabolic steroids, masculinizing tumors)
- Liver failure (decreased synthesis by liver), nephrotic syndrome (loss in urine), or malnutrition
- Hyperthyroidism (decrease in available binding sites on TBG)
- Sick patients with a variety of acute and chronic illnesses
- Drugs (glucocorticoids)
Serum TSH (Thyroid Stimulating Hormone)
TSH positively regulates thyroid hormone synthesis and release while a a negative feedback exists by thyroid hormone on TSH secretion by the pituitary.
Serum TSH is the best SCREENING test for the diagnosis of hypothyroidism or hyperthyroidism in healthy ambulatory individuals. It is the initial test done to assess thyroid function and the only test needed if it is normal.
Serum TSH in patients with primary hyperthyroidism (which accounts for 99.9% of the cases of hyperthyroidism) is low. A very low value (<0.01) is diagnostic of hyperthyroidism while a low value (0.01-0.1) suggests hyperthyroidism. Exceptions include conditions that primarily affect the hypothalamus/pituitary.
Serum TSH is invariably increased in patients with primary hypothyroidism (which accounts for 99% of cases of hypothyroidism) and is one of the most specific tests in medicine; virtually nothing else raises the serum TSH.
Hypothyroidism
Epidemiology/Pathophysiology
The incidence of hypothyroidism varies based on sex, age and geographic/environmental factors (most important being dietary iodide), but over 5-10% of individuals over 65 may have hypothyroidism. Hypothyroidism can occur as a result of a defect within the thyroid gland itself (primary hypothyroidism) or from a deficiency of TSH secretion (secondary hypothyroidism) or TRH secretion (tertiary or hypothalamic hypothyroidism). Thyroid insufficiency can also arise from peripheral tissue resistance to thyroid hormone. The treatment of hypothyroidism is oral thyroxine (T4). Secondary hypothyroidism may be treated with additional medication
Primary Hypothyroidism
Primary hypothyroidism is due to defect within the thyroid gland. This is by far the most common cause accounting for 98% of cases of hypothyroidism.
Chronic Thyroiditis (Hashimoto's)
Chronic thyroiditisis almost always due to Hashimoto's thyroiditis which is the most common cause of hypothyroidism. The etiology of Hashimoto's thyroiditis is autoimmune destruction of the thyroid gland. Similar to other autoimmune conditions, Hashimoto's is more common in women with age. There is a strong familial component. Thyroid destruction is irreversible and slowly progressive. Thyroid antibodies (anti-thyroglobulin and/or anti-TPO antibodies) are present in the majority of patients. Autoimmune thyroiditis may coexist with other autoimmune disease such as pernicious anemia, rheumatoid arthritis, and diabetes mellitus. "Burnt out" Graves' disease also belongs in this category.
Secondary Hypothyroidism
In adults, it is almost always due to pituitary disease. These patients often have other associated pituitary dysfunction. Selective TSH deficiency is a very rare genetic cause of newborn hypothyroidism and may also be seen in adults.
Clinical Findings of Hypothyroidism
Hypothyroidism may be suspected by symptoms and signs, but the diagnosis needs to be confirmed biochemically (laboratory testing).
The most common features of hypothyroidism include fatigue, dry skin, cold intolerance, constipation, menstrual irregularities and possibly weight gain.
The skin appears pale and waxy due to vasoconstriction, increase in carotene concentration and anemia. Coarse dry hair and hair loss especially from the temporal aspect of the eyebrows. Decreased activity of sebaceous glands contributes to the dry skin
Bradycardia, impaired muscular contraction and decreased cardiac output are seen. Cardiomegaly and pericardial effusion may be present. Pleural and peritoneal effusions also may be encountered. Angina may occur due to coronary artery disease upon initiation of thyroid replacement. There is evidence to suggest that incidence of coronary atherosclerosis is elevated in hypothyroidis. Dyspnea and anemia is common. Appetite is reduced. Modest weight gain may be seen due to water retention.
Thyroid hormone is essential in nervous tissue development. Children born hypothyroid suffer from severe brain damage (cretinism). The earlier the initiation of treatment, the better the results for normal intellectual development. Decreased concentration, lethargy and coma may be seen in adults. Sedatives (morphine, barbiturates, etc.) may precipitate C02 narcosis and coma. Carpal tunnel syndrome may be seen. Reflexes are characteristically slow (relaxation phase) due to decreased muscle function. Muscle stiffness, aching, cramps very common. Lack of thyroid hormone during development can result in skeletal deformity and can have similar effects of degenerative arthritis in adults.

Hyperthyroidism
Hyperthyroidism refers to excess thyroid hormone from hyperactivity of the thyroid gland (excess production or release). This is called thyrotoxicosis.
Graves' disease is the most common form of hyperthyroidism accounting for 60-70% of all cases. It occurs in up to 3% of the population. There is a strong familial component and the disease is more common in women (F:M ratio 5:1) in the third and fourth decade. It is an autoimmune disorder.
The symptoms and signs of hyperthyroidism, shown in Table 1, and their severity correlates with the level of circulating thyroid hormone.
| Table 1. Symptoms and Physical Signs of Thyrotoxicosis | |
| General | Weight loss, heat intolerance, insomnia |
| Skin | Sweating, palmar erythema, onycholysis (nail separation from nail bed) |
| Nervous System | Tremor, Nervousness, anxiety, hyperkinesis |
| Cardiovascular | Dyspnea on exertion Palpitations, arrhythmia (atrial fibrillation) Increased systolic BP, decreased diastolic BP, Increased cardiac output |
| Reproductive | Irregular menses, amenorrhea, infertility |
| Gastrointestinal | Increased frequency of bowel movements |
| Musculoskeletal | Myalgia, proximal muscle weakness Osteopathy (subperiosteal bone formation and swelling) |
| Head and Neck | Lid lag, stare, lid retraction Goiter |