PT Examination and Evaluation
History: Includes positions and movements which increase and/or relieve pain, duration of symptoms, level of irritability, pattern during the day/night, pain quality and location, onset and history of previous episodes.
May include self-report questionnaires to quantify level of pain and/or disability due to lumbar symptoms; can be used to differentiate between physical findings and psychosocial contributors to pain presentation.
Red Flags
During the examination, the PT will review the patient's history to rule out evidence of serious medical pathology. PTs use a systems review process to confirm the condition is within the scope of practice of physical therapy:
- Violent trauma
- Constant, progressive pain that does not change with movement or position
- Thoracic pain
- history of carcinoma, steroid use, drug abuse
- HIV
- Unexplained weight loss
- Persistent severe restriction of lumbar flexion
- Widespread neurological symptoms
- Structural deformity
Musculoskeletal
7 minute video
![]()
2 minute video
![]()
- postural deviations may indicate mobility restrictions (joint, muscle, etc)
- PTs may assess a patient's ability to self-correct postural deviations with verbal and/or tactile cues
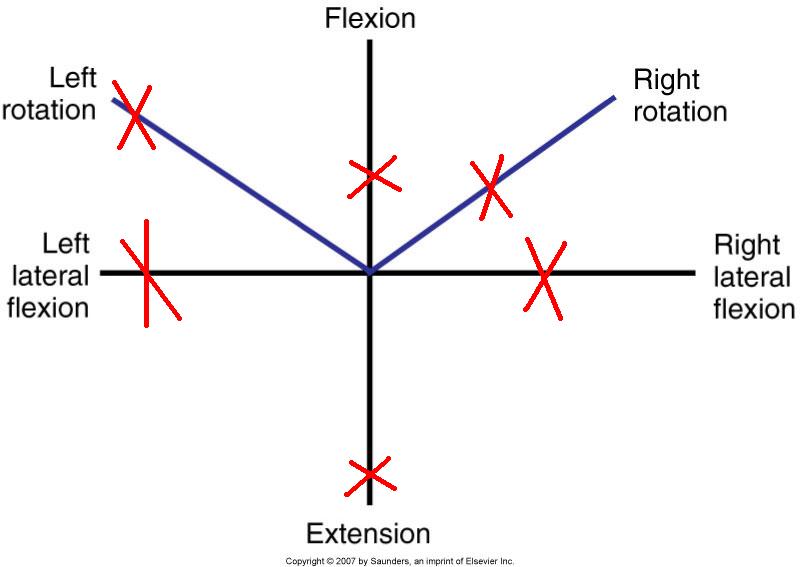
- Range of motion is the primary impairment in LBP and is used to evaluate response to treatment. PTs may use a visual scale to document AROM as it relates to normal values. PTAs consult the evaluation for visual or quantitative assessment of spinal ROM
- ROM includes assessing response to overpressures when AROM and repeated AROM are pain-free or minimally symptomatic. The PT will apply gradual manual force to the spine in its end-range to provoke or clear symptoms with each spinal motion or with combined spinal motions (e.g., flexion + rotation R)
- Accessory segmental spinal motion is assessed and is classified as normal, hypomobile, or hypermobile
- abbreviated as PPIVM (passive physiological intervertebral mobility)
- hypomobile: benefits from mobilization, manipulation, stretching and stretching of related muscles
- hypermobile: benefits from stabilization
- Muscle length: often coincides with ROM testing; includes length of muscles which originate or insert on the spine/pelvis
- Muscle strength: MMT and functional tests are used to determine nerve root involvement and may provide information on secondary muscle guarding influences due to pain/perception of pain
- Mechanical Provocation Tests
7 minute video
![]()
- used by the PT to determine motions and involved structures which reproduce patient's primary complaint
- Quadrant/Foraminal closure test
- Spurlings is a combination of cervical SB + extension + axial compression + overpressure
- Positive (+) Spurlings is an indicator of cervical intervertebral disc or foramen dysfunction (radiculopathy)
- Cervical Compression
- Pressure is applied through the top of the head (axial loading)
- Positive (+) cervical compression is an indicator of nerve root impingement
- Cervical Distraction
- Cephalad manual traction is applied through the occiput
- Positive (+) cervical distraction test is reported when patient's symptoms decrease during traction and indicates cervical radiculopathy

Neuromuscular
- Pain: PT palpates painful and related structures, noting for warmth and tissue reactivity
- Peripheral nerve integrity: assessed through sensation testing and MMT for spinal dermatomes and myotomes respectively
- Reflex integrity: DTRs which are exaggerated, diminished or absent indicate spinal or other nervous system pathology
- Neurodynamic tests: Involves applying mechanical stress (stretch) to nervous tissue to distinguish nerve root compression and peripheral neuropathy contributors to patient's complaint
- Straight leg raise (SLR): Positive (+) indicates involvement of lumbosacral nerve roots. The PT should note the degrees of hip flexion when symptoms are elicited. Symptoms can present unilaterally, contralaterally or bilaterally. The PT may include medial hip rotation, hip adduction, ankle dorsiflexion, and/or cervical flexion to increase tension on nerve tissue.
- Prone knee flexion: Positive (+) indicates L2 and/or L3 involvement; may also produce SI pain due to restrictions in the rectus femoris
- Slump test: Positive (+) indicates lumbosacral nerve root compression or lumbosacral nerve involvement
- Upper Limb Tension Test (ULTT): Positive (+) indicates involvement of nerves in the brachial plexus. Movement tests are specific to radial, ulnar and median nerves
Special Tests
- Vertebral artery test: Positive (+) indicates evidence of vertebral artery compromise with end-range cervical motions, especially rotation and extension. High velocity joint manipulation or end-range motions are contraindicated
- SI Joint tests
- Abnormal SI mobility is classified as sacroiliac (abnormal positioning of sacrum on a normally positioned ilium) or iliosacral (abnormal positioning of the ilium on a normally positioned sacrum)
- Standing flexion test: Positive (+) if the PSIS moves upward (cephalad) and forward during lumbar flexion with respect to the contralateral side. Indicates restricted mobility of ilium on sacrum (iliosacral problem)

Sacral fixation test/Gillet's Test: Positive (+) if there is no PSIS movement as one hip flexes toward the trunk (iliosacral problem) (Approximately 1 minute)
![]()
Sitting flexion test: Positive (+) if PSIS moves cranially as trunk flexes forward (iliosacral hypomobility) (Approximately 30 seconds)
![]()
- Long sitting test: Used to determine abnormal rotation of the innominate on the sacrum
- moving from supine to long sit --> limb appears to lengthen in long sitting--> indicates posterior innominate rotation
- moving from supine to long sit --> limb appears to shorten in long sitting --> indicates anterior innominate rotation
- Compression tests: Positive (+) if manual compressive forces applied in supine to the SI joint(s) reproduce pain complaint
- Limb length inequality: Positive (+) if observed asymmetries with bony landmarks can be minimized or eliminated with placing blocks or shims under the shorter limb
- Prone instability test: Positive (+) if low back pain is reproduced with joint mobilization during active recruitment of lumbar extensors
- Thomas test: Positive (+) if hip flexion is greater than 0 degrees when controlled for lumbar extension. Indicates decreased mobility of hip flexors

Demonstration of Cervical Stabilization Progression
6 minute video
![]()
