
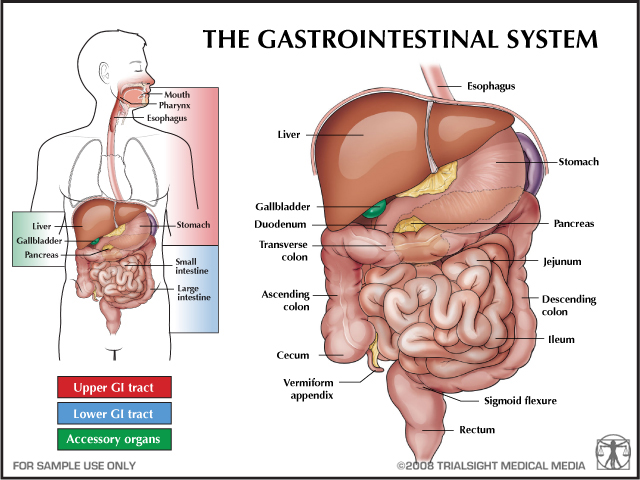
Gastrointestinal (GI) Health Conditions
Common Causes
- Infections
- Autoimmune/immuno suppressive's
- Genetic pre-disposition
- Lifestyle related: smoking, alcohol consumption (EtOH use), diet, stress
- Cancer
- Trauma
- Abdominal surgery: acute or history
Common Signs and Symptoms
- Nausea
- Vomiting (emesis)
- Anorexia
- Diarrhea
- Constipation
- Fluid and electrolyte imbalances
- Pain - abdominal and pain referred to abdominal region from another primary source
- Malnutrition
Common Treatments for GI Problems
- Dietary modifications: reduction of nicotine, caffeine, alcohol
- Stress reduction
- Drugs
- Laxative
- Anti-diarrhea
- Antacids
- Analgesics
- Anti-emetic
- Surgical
- Gastric bypass
- Gland removal
- Bowel resection for bowel obstruction
- Hernia repair

A pharmacological approach to some gastrointestinal problems is appropriate in some cases
Patient support equipment
Intravenous (IV) lines
- IV fluids administration
- Total Parental Nutrition (TPN - IV delivery of food and nutrients)
- Red blood cell infusions
Nutritional support
- Percutaneous endoscopic gastronomy (PEG) tube
- Nasogastric (N-G) tube
- Red blood cell infusions
Fluid drains
Active drains use suction to remove fluids
• Jackson-Pratt drains (JP) – closed drain (has a collector) that aids in removing fluid from abdominal wounds.

Drains to remove fluids post surgery
https://upload.wikimedia.org/wikipedia/commons/1/10/Post-operative_Jackson-Pratt_Drains.JPG
• Sump drains – open drain that also removes fluid by suction
Passive drains use pressure differentials and/or gravity to remove fluid
• Foley catheter - indwelling tube that collects urine
• Colostomy bag - external bag that collects fecal waste

https://commons.wikimedia.org/wiki/File:Ileostomy_with_bag.jpg

Common Classification of GI Dysfunction
![]()
Guided Learning #1. Guided learning to assist in table below and Goodman reading: just
over 10 min.
|
Anatomy |
Pathology |
Associated Terms |
Risk Factors |
Signs and Symptoms |
|
Upper GI |
Candidiasis Yeast Infection
|
Thrush |
Antibiotic use Immuno-suppression
|
Red, swollen mouth with white patches that can be scraped off Weigh loss due to pain in mouth with eating
|
|
Upper GI
|
Herpes Simplex 1 Viral Infection |
Cold Sore Fever blister
|
Contact by mouth with carrier/host
|
Burning blister in and around mouth. |
|
Upper GI |
Dysphasia |
Aspiration |
Neuromuscular impairment GI Disease
|
Difficulty with safe and effective, chew and swallow Coughing with eating and/or drinking
|
|
Upper GI |
Gastroesophageal reflex disease (GERD) Reflux of gastric contents into stomach
|
Acid Reflux Barium Swallow Endoscopy
|
NSAID use alcohol use. Infection. Smoking/tobacco use. Excessive acid production
|
Heartburn Regurgitation Esophagitis Dysphagia Pain (sub-sternal, non-cardiac) Sore or hoarse throat Hematemesis
|
|
Upper GI |
Barrette's Esophagus Change in epithelial cell morphology
|
Chronic GERD |
Alcohol use and smoking, chewing tobacco use may lead to esophageal cancer
|
Same as GERD with increased severity
|
|
Upper GI |
Esophageal Cancer
|
Squamous carcinoma Achalasia Stricture
|
EtOH/alcohol abuse. Smoking. Diet imbalances
|
Same as GERD, with increased severity, weight loss, pain
|
|
Stomach |
Gastritis Inflammation of inner stomach layer (mucosa) Can lead to electrolyte imbalance
|
Dyspepsia |
Trauma Salmonella infection NSAID Aspirin Alcohol related renal failure Liver failure Mechanical ventilation >48 hrs
|
Hemorrhage Fever Epigastric Pain Nausea Anorexia Hematemesis
|
|
Stomach |
Peptic Ulcer Disruption of the gastric or duodenal mucosa
|
Bleeding Perforation Obstruction
|
Excessive alcohol use Diet Stress NSAIDs Bacterial infection
|
Burning, gnawing pain Reduction of pain with eating Burping Nausea and/or vomiting Bleeding
|
|
Lower GI
|
Irritable Bowel Syndrome (IBS)
Colon Dysfunction |
BRAT diet (banana, rice, apple, tea or toast)
|
Stress Decreased sleep Dietary exacerbations (wheat, rye, barley, milk, EtOH, caffeine)
|
Alternating loose stools and constipation Bloating with abdominal pain Cramping Mucous/blood in stool
|
|
Lower GI |
Crohn's Disease Inflammation of intestinal wall
|
Ileitis Enteritis
|
Unknown Possible autoimmune response to bacterial or viral infection
|
Abdominal pain Diarrhea Occasional. Rectal bleeding Weight loss Small bowel obstruction Fistula formation Nutritional Deficiencies
|
|
Lower GI |
Ulcerative Colitis Inflammation of colon and /or rectum
|
Inflammatory bowel disease
|
Unknown Possible autoimmune response to bacterial or viral infection
|
Alternating loose stools and constipation Bloating with abdominal pain Cramping Mucous/blood in stool
|
|
Intestinal |
Whipples Disease
Bacterial mal absorption condition
|
Malnourishment
|
Exposure to Tropheryma Whippelli
|
Abdominal pain Weight loss Incomplete breakdown of intestinal materials Diarrhea Intestinal bleeding Fatigue and Weakness
|
|
Intestinal |
Short Bowel Syndrome Disorder from surgery where >50% of small intestine is removed Mal absorption condition
|
Total Parenteral Nutrition (TPN) |
History(Hx) of abdominal surgery Crohn's IBS Intestinal Trauma
|
Weakness Fatigue Depression Dehydration Weight loss Diarrhea Cramping and bloating Heart burn Weight Loss Diarrhea Malnourishment
|
|
Intestinal |
Diverticulosis Small outpourings or hernia in intestinal wall
|
Diverticulitis Intestinal necrosis
|
Advanced age Low fiber diet |
Abdominal pain Fever and chills Nausea and vomiting Cramping Constipation Fistula formation
|
|
Intestinal Bowel & Abdomen |
Ostomy Surgical opening from bowel or intestine to the outside. |
Ileostomy (removal of colon and rectum) Colostomy (removal of colon)
|
History of cancer, intestinal disease Trauma
|
External pouch for collection and elimination of waste
|
|
Intestinal and Abdominal |
Hernia Abdominal protrusion through a weak area in the abdominal wall
|
Inguinal (groin) Abdominal Femoral Hiatal Hernia or hernioplasty (reduction hernia and abdominal reinforcement)
|
Obesity heavy lifting straining during bowel movements Pregnancy Impaired nutrition Placement of abdominal drains General debility
|
Groin pain Palpable lump in groin Bowel obstruction Relief with applying pressure to bowel area/rectum or lower abdominal area. Shortness of breath
|
|
Vascular |
Hemorrhoids |
Sitz Baths |
Age (>50 yrs) Straining during bowel movements Chronic constipation
|
Pain Discomfort in sitting Itching Bleeding (anal canal and/or rectum)
|
|
Liver |
Jaundice Excessive bile production
|
|
Cirrhosis Hemolytic anemia
|
Yellowing of skin, eyes and fingernails
|
|
Liver |
Cirrhosis Fibrosis of liver tissue
|
Fatty liver. Alcoholic |
Hepatitis B, C, D Drugs and infection Autoimmune hepatitis
|
Effects multiple body systems |
|
Liver |
Hepatitis Inflammatory process in the liver; typically viral
|
Blood born pathogen
|
Viral infection EtOH/alcohol abuse
|
Effects multiple body systems
|
|
Gall Bladder |
Cholelithiasis
|
Gallstones |
Gender (Female), hx of diabetes, obesity. Ethnicity/higher in Native American and Hispanic communities versus African American/Caucasian.
|
Severe epigastric or right upper quadrant pain Referred pain under the right scapula Indigestion after eating fatty foods Nausea and/or vomiting
|
|
Pancreas |
Pancreatitis Inflammation of pancreas
|
|
EtOH/alcohol abuse, calcium malabsorption. Infection Abdominal trauma
|
Abdominal Epigastric pain (worse with walking, supine, eating) Abdominal swelling Nausea or vomiting Fever Dehydration Hypotension Pain radiating to low back |
Guided Learning #2 Liver Associated Health Conditions Guide to Goodman Readings
Just over 13 min
![]()
Guided Learning #3 Pancreas and Gall Bladder Associated Health Conditions Guide to Goodman Readings
Just over 7 min
![]()


Obesity
Classified by Body Mass Index of >+30kg/m2
- Large population based studies show that for every additional 5 BMI points (from between 20-25kg/m2), there is a 39% increase in risk of death due to weight contributors
- Premature risk of death rates are higher in younger people and men with obesity
- Death from stroke, respiratory disease, and heart disease increases in people with BMI over 25kg/m2
Do you know your Body Mass Index? Calculate it here
![]()
![]()
![]()
![]()
- second most preventable cause of death (smoking is first)
- metabolic syndrome starts in utero before a child is born
- consumption of sugar by parent/mom due to:
- ready access to inexpensive and portable foods
- poverty and resultant lack of access to healthy food.
- children who experience food insecurity are more likely to develop obesity (Kaur, Lamb, & Ogden, 2015)
- education in healthy eating, calorie consumption, and its resultant effects can have a significant influence in obesity rates in children and parents
Disease risk factor increases related to obesity
(Lustig, Brindis, & Schmidt, 2012)
- – Type II diabetes
- – hypertension
- – coronary artery disease
- – cerebral vascular accident
- – osteoarthritis
- – asthma
- – obstructive sleep apnea
- - Erectile dysfunction (males)
People with obesity are more likely to have malignancies in the GI tract as associated with the cause of death (Saab & Salvatore, 2015)
Psychosocial Obesity Affects

Image represents the relationship between mental health
and the health condition related to the gastrointestinal system
• decline in function due to restricted activity
• musculoskeletal pain (bone and joint)
• negative health perception
• anxiety and depression - including in children and adolescents
• increased personal health care costs
• increased incidence of disability
• increased discrimination and abuse
• increased risk for negative or biased health care decisions from health care providers (Casazza, et al., 2013).
• decreased access to treatment spaces and medical equipment during encounters with providers (e.g., BP cuffs, gowns, exam tables, scales)
Weight Loss Effects
• 5-10% reduction can produce measurable health benefits
• Decreased absenteeism from work reported from surgical and non-surgical weight loss programs
• Patients who are morbidly obese (BMI > 40 kg/m2, or 100 pounds over ideal weight) may qualify for bariatric surgery (gastric bypass) for weight control
Physical Therapy Role

PT Examination and Evaluation
The physical therapist prioritizes interventions within the physical therapy plan of care by integrating knowledge of body structure and function, participation restrictions, and contextual factors that inform prognosis and physical therapy diagnosis. Patient education in lifestyle factors that influence GI system disease should be integrated into a plan of care, with collaborative coordination with the medical and behavioral healthcare team as indicated. Patients with GI dysfunction may often present with co-morbidities in the integument, cardiopulmonary, and musculoskeletal systems. Physical therapy providers should self-assess and seek opportunities for professional development specific to metabolic and GI dysfunction in order to minimize bias and reduce negative perceptions of patients in this population.
PT/PTA Relationship

A strong PT/PTA or inter professional team will result in a more positive outcome
for the patient
• Maintain positive, open, timely, patient-centered communication
• Delegate and accept responsibilities for treatment based on the skill level of the PTA
• POC
– PT: Modify and update POC based on progress reported or reassessment
– PTA: Document patient status (progress/barriers) and request clarification or input as needed depending patient response and skill set
Role of the PTA
Tests and Measures

A ROM assessment is part of the musculoskeletal system overview
hen treating a pt. with a gastrointestinal health condition
Aerobic Capacity and Endurance
- VS pre- post- activity, Borg RPE, O2 sats, observation for s/sx of cardiopulmonary response
Anthropometrical Characteristics
- Height, weight, BMI, edema measures
Arousal, attention, cognition
- A&O, memory and recall
Pain
- VAS, faces scale, location, referral patterns
Joint Integrity and Mobility
- Range of motion(PROM/AROM) extremities and trunk
Neuromuscular tests
- Sensation and reflexes
- Strength
- Coordination
Functional Activity Performance
- FIM, Oswestry Disability Index
- Gait and locomotion
- Bending, lifting, carrying, reaching
Interventions for decreased endurance/aerobic capacity

Transfer training may be part of the plan of care for a pt with a gastrointestinal health condition
1. Log rolling/bracing with pillow
2. Transfer training
3. Endurance training (gait, exercise)
4. Postural training
Interventions for impaired ventilation/respiration

Incentive spirometers may be used
especially in the acute setting for respiratory health for a pt with
a gastrointestinal health condition
1. breathing exercises
2. incentive spirometry
3. huffing/directed cough
4. chest percussion and vibration
Interventions for Impaired integument integrity
1. Wound care for incisions
2. Skin/wound care for ostomies
3. Generalized skin care and education skin inspection for at-risk areas
Interventions for Decreased ADLs and Self-Care
1. Training in adaptive devices and equipment
2. Environmental assessment and modifications
Interventions for Disability Prevention and Wellness

Shoulder ROM and breathing exercises can help
prevent other health conditions
Education in
1. Lifestyle modification/decreasing risk of recurrence
2. Energy conservation (pacing and prioritizing)
3. Ostomy care
